

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Kidney transplantation is an appropriate treatment for end-stage renal disease (ESRD) in patients needing continuous hemodialysis [1]. The demand for living donors has increased with the incidence of ESRD and the absence of a cure other than transplantation. As a result, expansion of the living donor pool is a challenge. Living donor nephrectomy involves major kidney surgery on a healthy donor to treat another individual. The donor can be exposed to the risk of complications related to the donor nephrectomy. In addition, some studies have reported that complications of the procedure tend to be underreported [2-4]. However, prospective living donors must receive, before surgery, an accurate description of the long- and short-term risks associated with the procedure. Providing such information may be complicated by the recent development of various surgical techniques designed to reduce the risk of complications. These techniques include laparoscopic living donor nephrectomy (LLDN), hand-assisted laparoscopic donor nephrectomy (HALDN), and video-assisted minilaparotomy surgery-living donor nephrectomy (VAMS-LDN) [5-10]. Prospective donors should be systematically and accurately informed of the advantages and disadvantages of each surgical technique and its risk of complications so that they can choose the procedure that is most appropriate for their economic and individual circumstances.
The complications of surgeries were first systematically classified by Clavien et al. [11] in 1992 in relation to cholecystectomies. The classification system included four grades and became widely used for various types of surgeries [11-14]. In 2004, life-threatening complications and long-term disabilities were added to the classification and duration of hospital stay was eliminated as a variable in grading. The modified Clavien classification is now the most commonly used system worldwide for various types of surgeries [15-20].
Several authors have also attempted to apply this classification in reporting the complications of living donor nephrectomies. Kocak et al. [21] analyzed 43 complications of LLDN in 600 cases and reported the outcomes of their modified Clavien classification. In 2010, Harper et al. [22] published the analysis of complications of 750 cases of LLND by use of the same modified classification.
In our institution, VAMS-LDN has been conducted for living kidney donors since 1993 and has been widely applied since the blade-to-the-table-mount retractor system (Thompson Surgical Traverse City, Inc, Traverse, MI, USA) was invented in 2002 [23]. VAMS-LDN is a surgical technique combining the advantages of open donor nephrectomy and laparoscopic donor nephrectomy and can characteristically provide a surgical space without muscle dividing. As a result, it can provide the surgeon with direct vision through a minilaparotomy incision site and a magnified vision through the telescopic view when performed with a surgical traction system. If a problem occurs, the procedure can be converted to open surgery immediately. Compare with other laparoscopic techniques, VAMS-LDN carries a lower risk of reduced urine output and cardiovascular complications because it does not require a pneumoperitoneum. Moreover, it is reported to be safe and associated with low morbidity rates [23].
In the present study, we analyzed the complications of VAMS-LDN cases with use of the modified Clavien classification system to demonstrate the low complication rate of VAMS-LDN.
MATERIALS AND METHODS
We retrospectively investigated 720 VAMS-LDN cases conducted at our institution by two surgeons from 2003 to 2010. The complications were divided on the basis of Dindo's version of the Clavien classification, which is a modified Clavien classification. The modified classification was designed for LLDN, and VAMS-LDN is an open surgery technique. However, we used the classification to compare our complication rates with those of Kocak et al. [21] and Harper et al. [22] who studied the complication rates of LLDN in many patients. Dindo's version of the Clavien classification was used not to describe intraoperative complications, but to describe postoperative complications. The study was approved by the hospital Institutional Review Board.
Collected data included height; weight; body mass index (BMI); age; sex; smoking history; medical history positive for hypertension, diabetes mellitus, mild anemia in females (hemoglobin 10 to 11 g/dl), or mild dyslipidemia (total cholesterol 220 to 270 mg/dl or triglyceride 150 to 200 mg/dl); previous surgery history; side of nephrectomy; vascular anomalies; multiple renal arteries; early bifurcation of renal artery; multiple renal veins; retroaortic renal vein; other vessel anomalies (i.e., gonadal vein anomalies, lumbar vein anomalies, aberrant vessel, double inferior vena cava and inferior vena cava); duplicated ureter; warm ischemic time; and operative time. Donor anatomy was assessed with multidetector computerized tomographic angiography/urography with reconstructions. Early bifurcation of the renal artery was defined as branching within 1 cm of the aorta for left-side donors and proximal to the right wall of the inferior vena cava for right-side donors. A modified Clavien classification of surgical complications was used. All prospective donors were evaluated by gastroenterologists, nephrologists, psychiatrists, and the donor surgical team at our institution.
RESULTS
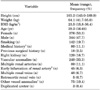
Patient characteristics are summarized in Table 1. The 720 donors consisted of 376 (53.3%) females and 344 (47.7%) males. The complications were divided on the basis of the modified Clavien classification designed by Kocak et al. [21]. The modified classification was designed for LLDN, and VAMS-LDN is an open surgery technique. However, we used the classification to compare our complication rates with those of Kocak et al. [21] and Harper et al. [22] who studied the complication rates of LLDN in many patients. Of all of the patients, 142 (19.7%) had a history of smoking; 80 (11.1%) had a positive medical history for hypertension, diabetes mellitus, mild anemia in females, or mild dyslipidemia; and 18 (2.5%) had a previous surgical history. No donors had a history of diabetes mellitus. Mean ischemic time was 189 minutes (range, 60 to 380 minutes), and mean warm ischemic time was 197 seconds (range, 30 to 420 seconds).
A total of 67 intraoperative and postoperative complications occurred (Table 2). All vascular injuries were immediately repaired intraoperatively with polypropylene sutures and caused no apparent postoperative problems. Postoperatively, lymphorrhea was observed in 4 (0.6%) patients and was successfully managed in all cases by delaying drain removal. Postoperative transfusion was performed for 9 (1.3%) donors, who did not need additional transfusions or surgery. A lymphocele developed in one donor (0.1%) and required the insertion of a pigtail catheter. The complications were readily classified by using the modified Clavien classification. No complications were of grade 2c or worse. Fig. 1 summarizes the distribution of complications by grade and compares them with the findings of Kocak et al. [21] and Harper et al. [22].
DISCUSSION
Research using reproducible and systematic classifications of surgical complications is important for various reasons. Surgeons require the results of such research in choosing or recommending treatment strategies to patients and in managing complications when they occur. In addition, patients must be provided with adequate information before choosing whether to undergo a procedure. In many cases, the information should include details on the incidence of major versus minor complications and immediate postoperative versus long-term complications associated with each type of surgical technique available. A systematic classification can also reduce subjective interpretation and over-generalizing negative outcomes. Moreover, it can facilitate a systematic and rational comparison of treatment results among different centers and surgical techniques.
In 1992, Clavien et al. [11] classified the complications of open cholecystectomy. In 2004, a modification of the existing classification was developed as a result of an extensive cohort study and survey including 6,336 patients [15]. This modified Clavien classification is now widely accepted and used in clinical and research settings.
Living donor nephrectomy is a surgical procedure with no clinical advantage for donors; therefore, the assessment of complications is of primary importance in outcome assessment. Patients who undergo a living donor nephrectomy are exposed to the risk associated with having a single kidney and various other complications. Therefore, one must provide them with detailed and systematic information about complications. It is widely known that the quality of life of donors is not lower than that of non-donors. The probabilities of chronic complications are not significantly different between living donors and non-donor controls.
As mentioned, Kocak et al. [21] and Harper et al. [22] proved the safety of LLDN by analyzing its complications systematically by using the modified Clavien classification of surgical complications with 600 and 750 cases of LLDN in 2006 and 2010, respectively. In our institution, VAMSLDN has been performed since 1991, but a systematic analysis of its complications with well-organized criteria had not previously been performed. VAMS-LDN is a surgical technique that uses a smaller incision than that used in open surgery: a 5 to 7 cm incision along with a magnified view through a telescope. This technique provides the advantages of both laparoscopic and open surgery. Because it differs from LLDN, which has been widely performed, it carries a risk of different complications. To assess these complications, we retrospectively analyzed 720 cases of VAMS-LDN by using the modified Clavien classification.
We found an overall complication rate of 9.3% (67 complications in 720 patients). Most of these (49 [6.8%]) were grade 1 complications, and 16 (2.2%) were grade 2a complications. grade 2b complications occurred in 2 cases (0.3%), and complications of grade 2c or worse did not occur. Compared with an analysis of the complications of LLDN based on the modified Clavien classification in the two studies mentioned before, the rates of grade 1 and grade 2a complications were slightly higher in this study. The rates of grade 1 and 2a complications associated with VAMS-LDN at our institution were slightly higher than those associated with LLDN as reported by Kocak et al. [21] and Harper et al. [22]: grade 1, 6.8% vs. 2.8% and 3.6%; and grade 2a, 2.2% vs. 0.8% and 0.7%, respectively. However, grade 2b or more severe complications occurred much less frequently with VAMS-LDN (e.g., grade 2b, 0.3% vs. 2.0% and 0.8%). Furthermore, complications more severe than 2b did not occur in our study but did in the studies of LLDN. Because vascular injuries are especially important, we included an analysis of these injuries regardless of grade, including those resolved immediately during surgery, without postoperative sequelae. This is in contrast with earlier studies that analyzed only those vascular injuries that resulted in postoperative problems (e.g., grades 2b and 2c). In this study, vascular injuries of grade 1 (resolved during surgery) and grade 2 occurred 14 and 5 times, respectively. No vascular injuries of grade 2b or worse occurred. On the basis of these findings, which were derived by use of the modified Clavien classification, VAMS-LDN appears to be a safe procedure.
CONCLUSIONS
The results of the present study, which were derived with use of the modified Clavien classification, a systematic and standardized classification of surgical complications, suggest that VAMS-LDN is a safe procedure. The systematic evaluation of complications for living donor nephrectomy will likely enable patients to make more informed decisions and will enable medical staff to better manage complications and improve surgical techniques.


 XML Download
XML Download