

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Most intraperitoneal bladder ruptures result from blunt trauma. Impalement injury of the urinary bladder is extremely rare. Here we report a case of impalement injury with intraperitoneal bladder rupture secondary to perirectal impalement.
CASE REPORT
A 31-year-old man fell from 2 m in height while working at a construction site. He sustained an impalement injury through his perirectal region when he landed on a steel pipe with a diameter of 19 mm. He pulled the pipe out himself and was transported to our hospital by ambulance. Upon arrival at our emergency room, gross hematuria and abdominal pain were recognized. There was no history of previous urological disease, and his past history included only bubonocele and cerebral contusion.
The physical examination revealed a 2-cm diameter penetrating wound (impalement injury) with bleeding in the perirectal region around the anus (Fig. 1) and gross hematuria through the urethral catheter. In addition, pain and abdominal defense were recognized by palpation. There was no disturbance of consciousness and his blood pressure was normal. Initial blood examinations were generally normal except for the white blood cell (WBC) count, which rose to 10,200/µl. However, blood reexamination 1 hour after admission revealed hemoglobin to have dropped from 15.4 to 12.9 g/dl.
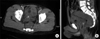
A computed tomography (CT) scan revealed hematoma around the perirectal space, suggesting rectal injury. Furthermore, a CT scan demonstrated a high-density area and free air in the bladder and that the posterior dome of the bladder wall was irregular, thus raising suspicion of a hematoma and a through-and-through bladder perforation from the rectal space (Fig. 2). Although the CT scan demonstrated neither obvious free air nor bowel injury, the existence of abdominal defense made us suspect intraperitoneal bladder rupture.
Because intraperitoneal bladder rupture was strongly suspected, we first performed explorative laparotomy to assess the bowel injury. Then, extended surgery was performed to repair the bowel injury that was recognized during laparotomy and to repair the bladder and rectal ruptures and to divert feces. The extended open surgery revealed a through-and-through bladder perforation: a 3-cm diameter intraperitoneal bladder rupture near the dome and bladder rupture with right ureter injury at the posterior wall. Also revealed were 3 distinct ileal injuries and rectal anterior trauma with communication to the bladder, anal injury, and a right seminal vesicle injury. The bladder injuries were repaired and a right ureterocystoneostomy was performed. To facilitate urine drainage from the bladder, bilateral single J ureteral stents, cystostomy, and a urethral catheter were placed. Partial ileectomy, rectal repair, and a diverting open loop colostomy with closure of the distal limb were performed. A part of the right seminal vesicle was ligated and cut because of injury and bleeding. The surgery time was over 10 hours. Total blood loss during the surgery was 7,205 ml, and blood transfusion of 6,820 ml was necessary in total.
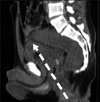
The black arrows in the figures indicate injury tracks confirmed by operative findings (Fig. 3). Therefore, we were able to diagnose intraperitoneal bladder rupture and bowel injury secondary to rectal impalement.
The patient's postoperative recovery was good. Thirteen days after the operation, retrograde cystography revealed no extravasation from the bladder. The patient was decatheterized and left our hospital 34 days after the operation. Two months later, intravenous pyelography showed smooth flow of the right ureter and no abnormalities of his ureterocystoneostomy and urinary bladder. Three months later, the colostomy was closed, and his feces were normal.
DISCUSSION
Bladder rupture is classified into non-traumatic and traumatic forms according to the cause. Non-traumatic rupture includes pathogenic and idiopathic ruptures. Traumatic bladder rupture reportedly accounts for 85 to 96% of bladder ruptures, although bladder injury itself is not common because the bladder is located deep in the pelvis [1,2]. More than 50% of traumatic bladder ruptures are reportedly associated with traffic accidents and pelvic fractures [1]. As in this case, impalement injury of the urinary bladder is extremely rare, accounting for less than 1% of all bladder injuries [3]. The majority of penetrating injuries are secondary to a gunshot wound; in particular, injuries secondary to rectal impalement are rare [4].
To our knowledge, 59 cases of impalement injury of the urinary bladder have been reported in Japan [5]. Over 60% of reported bladder injuries were associated with multiorgan injuries (Table 1). Approximately 15% of reported bladder injuries were associated with bowel injury, and these were intraperitoneal bladder ruptures. In diagnosing bladder rupture caused by impalement injury, multiorgan injury including intraperitoneal bladder rupture should be considered.
As in this case, rectal impalement injuries are rare and give us little information about the extent of the injury. It was reported that the most common secondary injury after such a rectal injury is injury of the genitourinary tract [6,7]. Therefore, extensive examinations, including examination of gastrointestinal and genitourinary injuries, are necessary. This case illustrates several key concepts in the diagnosis of bladder injuries. Gross hematuria, falling hemoglobin, and the existence of abdominal defense may aid in diagnosis. Retrograde cystourethrography, cystoscopy, CT, and so on are appropriate diagnostic studies in patients with suspected bladder injuries. In this case, a CT scan demonstrated bladder injuries but no obvious bowel injuries.
Many series of patients with extraperitoneal bladder rupture managed by a nonoperative or conservative approach have been reported [8]. Nonoperative management implies simple catheter drainage and clinical observation. However, operative management should not be delayed if intraperitoneal bladder rupture is suspected. Intraperitoneal bladder rupture should be repaired with absorbable sutures, and a perivesical drain, ureteral stent, and urethral catheter should be placed. Penetrating rectal injuries should be treated with fecal diversion, presacral drainage, distal rectal washout, and rectal wound repair. Colostomy is also necessary to prevent rectourinary tract fistulas [9]. In summary, impalement injury of the urinary bladder, especially secondary to rectal impalement, is extremely rare, and multi-organ injuries should be taken into account until injury is definitively ruled out. In addition to the examination and repair of the urinary tract injuries, it is essential for urologists to consult and cooperate with other clinical departments for repair of multi-organ injuries.


 XML Download
XML Download