

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The percentage of the global population that is over the age of 60 years has been estimated at about 10% and is expected to increase up to 20% by 2050 [1]. In Korea, a remarkable increase has also occurred in the percentage of the population aged >65 years, rising from 3.8% in 1980 to 9.5% in 2006 [2]. Lower urinary tract symptoms (LUTS) are highly prevalent among elderly men and women. For example, urinary incontinence affects 15 to 35% of the community-dwelling elderly and 22 to 90% of those in nursing homes [3,4]. LUTS not only affects quality of life but is also associated with significant morbidity of aged individuals, such as long bone fractures [5]. Moreover, LUTS is a significant contributor to the high socioeconomic cost of the management of both community-dwelling and institutionalized elderly individuals [6].
Most cases of LUTS are attributed to an overactive bladder or stress urinary incontinence (SUI) in women and to benign prostatic hyperplasia (BPH) in men; however, other age-related changes in the lower urinary tract are recognized in the elderly. Detrusor underactivity (DU) is one such age-related change in the urinary bladder. DU is defined as a contraction of reduced strength or duration, resulting in prolonged bladder emptying or a failure to achieve complete bladder emptying within a normal time span [7]. The prevalence of DU is considered to be high among the institutionalized elderly, especially in incontinent nursing home residents; DU is present in up to 80% of female nursing home residents [8]. Moreover, in older community-dwelling adults, in addition to the definitive voiding symptoms, DU has been related to a low rate of improvement in both individual symptoms and quality of life following prostate surgery in men or a mid-urethral sling procedure in women [9,10]. However, because no standard measurement techniques or quantitative diagnostic criteria have been developed, the prevalence and clinical implications of DU in the elderly population remain largely unknown. As a result, proper diagnosis and management of this condition is challenging for physicians caring for elderly patients with LUTS.
To date, several studies have reported the prevalence of DU among community-dwelling elderly suffering from LUTS, although there has been no standard definition of urodynamic DU [11-14]. However, these studies only considered small populations and did not evaluate the clinical characteristics of DU. Therefore, most of the relevant information regarding the clinical features of DU has been inferred from epidemiological studies of urinary retention [15]. To develop a greater understanding and to lay a foundation for further studies regarding DU, we tried to identify the prevalence and clinical features of DU in an elderly population presenting with LUTS.
MATERIALS AND METHODS
1. Patients and clinical data
We reviewed the computerized medical records of 1,817 patients aged over 65 years who had undergone a urodynamic study for LUTS at our institution between May 2003 and June 2010. The clinical data included demographic characteristics, types of urinary symptoms, free uroflowmetry and post-void residual (PVR) volume, and the findings of the urodynamic study. Of all the patients reviewed, 556 were excluded from the study population for the following reasons: a neurogenic abnormality that affected micturition function (n=279), a history of surgery on the lower urinary tract (n=103), an anatomical deformation of the lower urinary tract (e.g., pelvic organ prolapse degree ≥3 in women) or regular use of a catheter for urine drainage (n=75), and impaired general health that affected voiding or made the patients unable to perform daily tasks by themselves (n=99). The institutional review board of our institution approved the study protocol.
Before starting a urological work-up, we took a detailed history of the patient's LUTS and performed a physical examination. At our institution, patients presenting with LUTS document an International Prostate Symptom Score (IPSS) and a 3-day frequency-volume chart (FVC), including the Urinary Sensation Scale (USS), at every voiding [16] during the initial evaluation. Episodes of urgency were defined as those with a USS rating ≥3. Clinical urinary symptoms were divided into three categories: storage LUTS (episodes of frequency ≥8 per day, episodes of nocturia ≥2 per night, or episodes of urgency or urgency urinary incontinence ≥3 on a 3-day FVC), voiding LUTS (intermittency score ≥3, weak stream score ≥3, or straining score ≥3 on IPSS), and post-micturitional LUTS (incomplete emptying score ≥3 on IPSS). Free uroflowmetry (DABA, Endo tech, Seongnam, Korea) and measurement of PVR volume (BladderScan BVI-3000, Diagnostic Ultrasound, Brothel, WA, USA) were performed before the urodynamic evaluation. An imaging study of the upper urinary tract, urine cytology, or cystoscopy was performed on those patients with microscopic hematuria or if otherwise necessary.
2. Urodynamic evaluations
A multichannel urodynamic study (UD-2000, Medical Measures Systems B.V., Enschede, The Netherlands), including a pressure-flow study (PFS), was carried out after discontinuation of all drugs possibly affecting micturition function for at least 3 days, in accordance with the guidelines of the International Continence Society [17]. Bladder compliance was considered reduced when the ΔV/Δpdet was ≤20 ml/cmH2O, and the patients were regarded as positive for idiopathic detrusor overactivity (DO) if spontaneous or provoked involuntary detrusor contraction was observed in the filling cystometry [17]. During a PFS, patients were instructed to void in a standing or sitting position under quiet and relaxed circumstances. If the first voiding trial failed, an additional trial was performed, considering the possibility that the failure was due to cortical inhibition. However, patients who failed a second time or could not perform a PFS were excluded from the analysis (n=82).
In male patients, DU was defined as a bladder contractility index of less than 100 [18], for which the index was calculated from the results of the PFS according to the following formula: detrusor pressure at maximum flow rate (PdetQmax)+5 Qmax. Bladder outlet obstruction (BOO) was defined as an Abrams-Griffith (AG) number of 40 or greater, for which the AG number was calculated as PdetQmax-2 Qmax [19]. Female patients were classified as having DU when Qmax was 12 ml/s or less and PdetQmax was 10 cmH2O or less [20] and were diagnosed as having BOO when Qmax was 12 ml/s or less and PdetQmax was 25 cmH2O or greater with sustained detrusor contraction based on a PFS [21].
3. Statistical analysis
The collected data are presented as means±standard deviations or as percentages. In the retrospective analysis, a Student's t-test or a chi-square test was used to confirm statistical differences among the patient subgroups according to the types of variables. The IBM SPSS ver. 19.0 (IBM Co., New York, NY, USA) was used, and a 2-tailed p-value<0.05 was determined to indicate statistical significance.
RESULTS
During the study period, a total of 1,179 patients aged over 65 years without the aforementioned exclusion criteria underwent urodynamic studies for LUTS. Table 1 shows the clinicodemographic characteristics of all the patients. Data on clinical urinary symptoms were obtained from 1,055 patients (89.5%), which revealed that storage LUTS were more prevalent than voiding or post-micturitional LUTS in both sexes. Of the female patients, 58.2% presented with SUI symptoms.
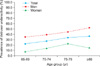
Urodynamic diagnoses are shown in Table 2. DO, DU, and BOO were more prevalent in men than in women, with a remarkable difference in DU prevalence between the sexes. Fig. 1 illustrates the prevalence of DU by age group. In both sexes, the prevalence of DU increased with age (p=0.053 and 0.002 in men and women, respectively), and the trend was more remarkable in women aged over 70 years. When the prevalence of DU was compared with the prevalences of DO, BOO, and urodynamic SUI (USUI) by age group, the prevalence of BOO was constant across the age spectrum, whereas the prevalences of DU and DO increased with age in men (Fig. 2A). In women, the prevalence of USUI decreased with age; however, the prevalences of DU, DO, and BOO increased with age (Fig. 2B).
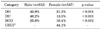
Table 3 compares the clinical characteristics between subjects with and without DU. Patients with DU were older than those without DU; however, types of clinical symptoms were not significantly different between patients with and without DU in either sex. Men with DU had a lower Qmax and a larger PVR volume during free uroflowmetry and had a lower prevalence of DO and BOO than did those without DU. In women, PVR volume was not significantly different between those with and those without DU. Women with DU had a lower first desire to void (FDV) volume and maximum cystometric capacity (MCC) and had a greater incidence of reduced compliance than did those without DU. The prevalence of DO was not significantly different between women with and those without DU. In men, 46.5% of subjects with DU also presented with DO or BOO; in women, DU was accompanied by DO or USUI in 72.6% of subjects with DU (Fig. 3).
DISCUSSION
The contractility of the bladder becomes impaired with age, which may result in the development of DU in both sexes. This age-related impairment is usually associated with structural changes in the detrusor muscle (dense bands), decreased axonal content, a reduced detrusor to collagen ratio, and changes in muscarinic receptors [22]. Although DU is thought to be a common geriatric condition, it has received little scientific attention. This is because the clinical characteristics of DU have not been clearly defined, and a gold-standard diagnosis for this condition has not yet been established from an urodynamic standpoint. Furthermore, the true prevalence of DU among the community-dwelling elderly remains largely unknown [15]. In this study, we aimed to elucidate the prevalence and clinical features of urodynamically proven DU in men and women over 65 years of age. To the best of our knowledge, there have been no studies on the relevant issues with large patient numbers.
We focused on patients who were over 65 years of age and were able to perform daily tasks by themselves. Patients who had neurogenic abnormalities that were presumed to affect micturition function or who used a catheter for urine drainage on a regular basis were excluded from the study population. We assumed that focusing on this population increased the clinical similarity of our study cohort with community-dwelling elderly as opposed to elderly in chronic care facilities, where over two-thirds of persons have been found to have DU [8]. In our study cohort, urodynamically proven DU was diagnosed in 40.2% and 13.3% of men and women, respectively. The prevalence of DU was similar to that of DO in men and increased with age in both sexes. We have not reached a conclusive explanation for the greater prevalence of DU in elderly men compared with elderly women. However, we believe that this phenomenon was related to the relatively higher prevalence of BOO [23,24] in men than in women in our cohort. However, because there was a lower prevalence of BOO among men with DU than in men without DU in this study, the reason for the greater prevalence of DU in elderly men than in elderly women is likely to be multifactorial.
The prevalence of DU in the elderly population in our study was similar to that reported in previous studies [11,13,14]. However, comparatively, the prevalence of DU in men reported by Abarbanel and Marcus [12] was relatively higher than in our study. We believe that this difference is because the population studied by Abarbanel and Marcus [12] was, on average, older than our study population and neurological diseases were present in up to 25.6% of the target population.
As for trends in the prevalence of lower urinary tract pathophysiologies among patients over 65 years of age, the prevalence of BOO was constant across the age spectrum, whereas the prevalences of DU and DO increased with age in men. In women, the prevalence of USUI decreased and the prevalences of DU, DO, and BOO increased with age. These findings imply that DU becomes a more important component of the pathophysiologies of LUTS in community-dwelling elderly, as well as in elderly in chronic care facilities, as the patients get older. In our male cohort, the constant prevalence of BOO across the age spectrum may be partly attributed to the exclusion of men with LUTS suggestive of BPH who received medication without a urodynamic study at the initial evaluation. In our female cohort, the prevalence of DU decreased in those over 80 years of age compared with those aged between 75 and 79 years, although the difference did not reach statistical significance (Fig. 1). We do not have an explanation for this phenomenon. However, in contrast with men, women over 80 years of age accounted for only 8.8% (n=48) of all women enrolled. Therefore, the difference may be ascribed to the relatively small number of women over 80 years of age.
The results of the present study revealed that half of the men and three quarters of the women with DU also had other pathologies such as DO, BOO, or USUI. Similarly, Abarbanel and Marcus [12] reported that two-thirds of the men and half of the women they studied with DU also had DO or low bladder compliance. This is an important observation for the clinical management of LUTS in elderly patients. The use of antimuscarinics for the treatment of DO may aggravate voiding difficulty and, consequently, may result in acute or chronic urinary retention in patients with DO and DU. Furthermore, in general, the elderly are more susceptible to developing adverse events from antimuscarinics; therefore, the clinical use of such medication for the treatment of LUTS should be implemented with more caution for elderly patients with DU. Likewise, the benefit for elderly patients from surgical procedures such as TURP for men or the midurethral sling procedure for women may be limited, with a relatively low rate of improvement in both symptoms and quality of life following these surgeries, especially when BOO or USUI coexists with DU [9,10]. Information on the presence of DU may be conducive to the development of appropriate counseling and treatment strategies for those elderly patients with LUTS who elect for surgical treatment.
Although not statistically significant, the prevalence of diabetes was higher in those without DU than in those with DU in the female population. We excluded patients who used a catheter for urine drainage on a regular basis, and the prevalence of diabetes was only 10.4% in women (Table 1). Therefore, in the present study, the effect of diabetes on detrusor function seems to be lower than that seen in diabetes cystopathy. Actually, the prevalence of diabetes did not differ significantly according to the presence of DU in either sex (Table 3). In our female cohort, subjects with DU had lower FDV and MCC than did those without DU. Because more women with DU also had reduced compliance compared with those without DU (a pattern not found in men), it is likely that DU is related to reduced bladder compliance, subsequently resulting in a lower MCC in the female elderly.
Symptoms alone may often be used to formulate a probable diagnosis and can serve as the basis for initiating conservative treatments. However, Bromage et al. [25] reported a poor correlation between symptoms and urodynamic diagnosis in elderly patients. Similarly, there was no relationship between type of LUTS and the presence of DU in males and females in our study (Table 3). This agrees with findings that have suggested that symptoms lack adequate precision for urodynamic diagnoses in case of other lower urinary tract pathophysiologies [15]. The results of this study suggest that urodynamic evaluation can help to avoid the unnecessary prescription of medication with potentially hazardous side effects. Clinical urodynamic investigation can offer more detailed information on lower urinary tract dysfunction and can aid in establishing strategies for the diagnosis and treatment of LUTS in the elderly community.
We used clear cut-off values for the diagnosis of DU or BOO on the basis of the PFS in women. However, contrary to their diagnosis in men, the diagnosis of DU or BOO in women represents a dilemma owing to the lack of established criteria. For the diagnosis of DU in women, we adopted the PFS cut-off values suggested by Gotoh et al. [20]. This set of criteria seems to be stricter for the diagnosis of female DU than the criteria used in previous studies [12,13]; however, more studies are needed in this area. The PFS criteria for BOO have previously been defined only for adult males [26]. Although some PFS criteria and nomograms for BOO have been developed for adult females, these have not been defined into standardized values [27]. The criteria for female BOO used in the present study [21] have been shown to be the more stringent among five contemporary urodynamic definitions of female BOO when correlated with clinical suspicion of BOO [28].
Our study had several limitations. First, our findings were derived from a single tertiary referral center. A multi-center, prospective study would be required to confirm our results. Second, owing to the retrospective design of the study, all patients who responded to initial treatments and who did not undergo a urodynamic evaluation were excluded from the study population. Finally, we excluded from the analysis patients who failed to void two times in a PFS or who could not perform a PFS. A recent study demonstrated that 84% of patients with acontractile detrusors during urodynamic study had detrusor contractions during ambulatory urodynamics [29]. Although the excluded patients accounted for only 5% of the total patients, the distribution of urodynamic diagnoses might have been affected by the addition of these patients with ambulatory urodynamics.
Considering the results of our study on the prevalence and clinical features of DU, physicians who manage elderly patients with LUTS should understand the age-related pathophysiological changes of the lower urinary tract and be aware that this population probably has DU. Further studies should make use of longitudinal trials, rather than cross-sectional trials, to identify the natural history of DU in the community-dwelling elderly.
CONCLUSIONS
DU is an important component of the pathophysiologies of LUTS in the elderly population, with prevalences of 40.2% in men and 13.3% in women, and becomes more prevalent with age. Half of the men and three quarters of the women with DU also had other pathophysiologies that can affect micturition function. Physicians who manage elderly patients with LUTS should understand the age-related, pathophysiological changes of the lower urinary tract and be aware that this population probably has DU, which can result in a low rate of clinical improvement following individual treatments.




 XML Download
XML Download