

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Retroperitoneal soft-tissue sarcoma is a rare disease that accounts for 10 to 15% of all soft-tissue sarcomas and 33% of all malignant retroperitoneal tumors. Among these, liposarcoma (LPS) is the most common histologic type [1-3] and is classified into 4 subtypes: well-differentiated (WD), dedifferentiated, myxoid/round cell (RC), and pleomorphic. Mixed-type LPS is rare and presents as two or more subtypes in a single tumor. Retroperitoneal liposarcoma (RPLS) is often asymptomatic and considerably large when initially diagnosed. Complete resection for curative intent is the treatment of choice, and a negative margin should be achieved to increase survival, even if resection of adjacent organs is needed [4-8]. Despite complete resection, local recurrence is frequent and leads to mortality. However, other treatments (chemotherapy and radiotherapy) have not been effective [2,9-13]. Besides the study of 21 Asians by Lee et al. [6], other RPLS studies have been based on Western populations. How RPLS in Asians compares with RPLS in Western populations has not been studied. This paper is a study of the surgical treatment and prognosis of RPLS in a single Korean tertiary medical center.
MATERIALS AND METHODS
Forty-eight patients with LPS were identified at our institute between July 1, 1984, and March 31, 2009. Fourteen patients not registered on the electronic medical record and 14 patients with surgical sites other than the retroperitoneum (e.g., extremities, testis) were excluded. One patient who did not revisit the hospital was also excluded. Nineteen patients were included in the current study. The patients' progression, outpatient records, operative notes, histopathological reports, and imaging studies were reviewed retrospectively. The study received Institutional Review Board and ethics committee approval.
RPLSs were classified into 5 histopathologic types according to the World Health Organization classification: WD, dedifferentiated, myxoid/RC, pleomorphic, and mixed-type [14].
The factors studied included age at diagnosis, sex, symptoms at presentation, histopathologic type, gross margin status, tumor size, tumor burden, disease recurrence after treatment, interval time from immediate previous surgery to disease recurrence, and treatment with chemotherapy or radiation therapy. In the immediate postoperative period, imaging studies (computed tomography [CT] or positron emission tomography) were conducted at 1 and 3 months. If there was no evidence of recurrence for 1 year, imaging was done after 6 or 12 months. Tumor size was defined as the maximum dimension on cross-sectional imaging for a solitary mass and as the sum of all maximum dimensions for more than one mass. Tumor burden was defined as the sum of 3 maximum tumor diameters. Morbidity and mortality analyses were conducted by reviewing charts and clinical records.
Statistics of survival and recurrence were analyzed by using the Kaplan-Meier method. The effect of prognostic factors on survival and recurrence was compared by using the log rank test.
RESULTS
1. Patient evaluation and demographics
Nineteen RPLS patients were evaluated. All patients underwent surgical treatment, and 35 total surgeries were done for curative purposes. The patient demographics are described in Table 1. The mean follow-up period was 66.8 months (range, 6 to 165 months).
2. Primary RPLS cases
Seventeen patients underwent their initial surgery at our hospital. The mixed subtype (52.9%) was the most common LPS, followed by WD (23.5%). Adjacent organ resection was performed in 10 patients (58.8%). The most commonly resected organs were the kidney and the adrenal glands (Table 2).
Four patients (cases 01 to 04) received adjuvant chemotherapy or radiation after the initial surgical treatment. Of these, case 01 was disease-free at 27 months and case 02 at 48 months after therapy. Case 01 received radiation therapy only and case 02 received 2 cycles of chemotherapy followed by radiation therapy. Case 03 was treated with adjuvant radiation therapy and had recurrent disease 17 years after the first operation. Reoperation was performed, and the patient has been disease-free for 4 months. Case 04 underwent 6 cycles of chemotherapy and had recurrent disease at 29 months after the initial operation. Reoperation was performed, followed by four additional cycles of chemotherapy. The patient suffered disease recurrence twice more, with each recurrence treated with surgical intervention without chemotherapy. Radiation therapy was applied 1 month after the third reoperation, and no recurrence was seen on an imaging study 1 month after radiation therapy. No recurrence has been seen at 61 months since the initial diagnosis.
3. Recurrent RPLS cases
Recurrent disease was confirmed by imaging in 9 of 17 patients. Among these 9 patients, cases 05 and 06 have been disease-free for 50 and 296 months after 2 and 3 rounds of reoperation, respectively. Case 07 underwent reoperation 5 years after the first surgery, and recurrence was suspected at 7 years after the initial diagnosis. This patient is under close observation with imaging studies at 3-month intervals, but no change has been seen for 1 year. As previously mentioned, cases 03 and 04 had recurrent disease after adjuvant chemotherapy or radiation therapy. Case 08 had disease recurrence twice (8 and 20 months after initial treatment) and underwent reoperation. Distant recurrence was seen on a CT image 1 month after the third operation, and adjuvant chemotherapy was initiated. After 8 cycles, partial response was achieved. A ninth cycle of chemotherapy was planned, but no further medical record exists.
4. Mortality and morbidity
A group of 3 patients (cases 09 to 11) had 2 cases of morbidity and 3 of mortality after surgical treatment. In case 09, incomplete initial resection presented as the mixed-type histology (myxoid/RC and pleomorphic), and adjuvant radiation therapy was administered. Seven months after treatment, disease recurrence was confirmed and 6 cycles of chemotherapy were administered. Disease progression and newly developed distant metastasis were seen on a follow-up CT scan, and the chemotherapy regimen was changed. After 1 cycle of the new regimen (15 months after the initial operation), the patient died of LPS progression.
Case 10 underwent wide excision and adjacent organs (left kidney, pancreas, spleen, adrenal gland, transverse colon, and duodenum) were resected. However, complete resection was not possible. Wound dehiscence and intestinal obstruction were observed after the first operation, and surgical intervention was done for the intestinal obstruction. After 17 months the LPS recurred, but reoperation was not possible due to the widely spread tumor and the patient's poor general condition. The patient died 29 months after the original diagnosis.
Case 11 initially underwent reoperation 3, 6, and 7 years after the initial treatment. During the fourth operation, complete resection was not possible. Bowel leakage developed and the patient died (8 years after the initial operation). Both of these latter cases were of the dedifferentiated subtype.
5. Survival, recurrence, and long-term survivors
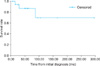
Average survival was 223.8 (±38.2) months and the overall survival rate was 84.2%. The 3- and 5-year survival rates were 86.9%, and the 10-year survival rate was 69.5% (Fig. 1).
Patients developed recurrence at a mean of 47.7 months. The mean time from initial surgery to first recurrence was 93 months. Recurrence occurred at a mean of 13.1 months after a previous imaging study (Table 3). The recurrence interval was significantly shorter in recurrent RPLS cases than in primary cases (p=0.023) (Fig. 2).
Recurrence of histopathologic subtypes was 60% for WD, 100% for dedifferentiated, 66% for myxoid/RC, and 44.4% for mixed-type RPLS. Among sex, age, histopathologic subtype, tumor size or burden, and resection of adjacent organs, there were no significant prognostic factors for recurrence or survival.
In several cases the recurred histopathologic diagnosis differed from the primary subtype. Cases 04 and 12, whose initial histopathologic subtype was WD, experienced recurrence of the dedifferentiated subtype. In case 06, the initial histopathology showed WD, but on recurrence the myxoid subtype was diagnosed after the first reoperation and the dedifferentiated subtype after the second reoperation.
Survival for more than 3 and 5 years was observed in 12 and 8 patients, respectively. Among these long-term survivors, 5 patients were reported to have mixed-type histopathology: WD and myxoid presented together in 4 patients (cases 05, 07, 13, 14) and myxoid and pleomorphic presented together in case 15. The histopathologic subtype of case 11 was the dedifferentiated type in all 4 surgeries. Case 04 was initially diagnosed as WD but subsequent histopathological reports after three reoperations showed dedifferentiated, mixed (WD and dedifferentiated), and WD, respectively. Case 06 underwent three surgeries, with each histopathologic result showing WD, myxoid, and dedifferentiated LPS.
DISCUSSION
RPLS is a rare disease and has a significantly better prognosis than other soft tissue sarcomas (leiomyosarcoma, malignant fibrous histiocytoma, malignant peripheral nerve sheath tumor, and hemangiosarcoma). Histological grade, resection margin, and tumor invasion of adjacent structures are known to affect RPS prognosis [1,3,15-19].
A study of 177 patients with primary RPLS operated on for curative intent by Singer et al. [4] reported disease-free survival rates of 73% at 3 years and 60% at 5 years. Histologic subtype, incomplete resection, and contiguous organ resection were associated with survival. When RPLS recurred locally, recurrence size, primary histologic variant and grade, and recurrence growth rate were independent predictors of disease-specific survival. For patients undergoing reoperation on locally recurrent RPLS, recurrence size and recurrence growth rate independently influenced the development of a second local recurrence, and repeated resection improved survival only for tumors with a growth rate of less than 0.9 cm/mo [20]. Of the patients studied, 56% presented with WD, 37% with dedifferentiated, 5% with myxoid, and 2% with RC RPLS. The dedifferentiated type was associated with a 6-fold increased risk of death compared with the WD type. Important prognostic factors for survival were incomplete resection, contiguous organ resection, and age >63 years. Nephrectomy was not associated with disease-specific survival; therefore, the authors proposed that kidney parenchymal sparing can be performed without influencing disease-specific survival [4].
Neuhaus et al. [5] reported a study of 72 patients who underwent surgical treatment for primary RPLS. More than half had excision of a continuous organ to achieve clearance. Direct tumor infiltration was seen in only 4% of patients. This supports the proposal by Singer et al. [4] of kidney sparing when possible. In this study, the authors did not see recurrence itself as an indication for further surgical treatment, and only surgery for palliative treatment was supported.
However, a study by Milone et al. [7] on 21 RPLS patients encouraged prompt surgical treatment for local recurrence. In that study, patients who had undergone complete resection of recurrent disease had a better mean survival than did patients who had not undergone complete resection. Therefore, a shorter follow-up interval was suggested for improved survival. Shibata et al. [21] also proposed that incomplete surgical resection, providing increased survival and symptom palliation, can be beneficial for selected patients with unresectable RPLS [1].
Although RPS is known to infiltrate the surrounding viscera, studies on RPLS have reported that direct organ infiltration is rare, suggesting a "pushing" character [5]. However, a recent study by Mussi et al. [19] reported that LPS involved 62.3% of resected viscera and that even WD, which is known to be least infiltrative, involved 48.6% of resected viscera. This may be why contiguous organ resection during surgery is negatively associated with local and distant recurrence and disease-free survival [4]. In our study, contiguous organ resection was not significantly associated with decreased recurrence. This was probably due to our limited sample size.
Treatment modalities other than surgical intervention such as chemotherapy and radiation therapy have not yet been established. Chemotherapy on LPS originating from the lower or upper extremities has been shown to be beneficial. The myxoid subtype is more chemosensitive, and ifosfamide has been shown to be more effective than doxorubicin [12,13]. No studies showing the effectiveness of chemotherapy on RPLS have been reported. Although some studies have reported that radiation therapy is beneficial for RPS, its effect on survival is still under debate. Morbidities due to toxicity on adjacent radiosensitive central organs remain an important obstacle [2,10,11,22-28].
Nearly all studies on RPLS have been based on Western populations. A recent report by Lee et al. [6] was conducted on 21 Asian patients. In these patients, 61.9% of the tumors were WD, 19% were myxoid/RC, 14.3% were dedifferentiated, and 4.8% had pleomorphic morphology. Surgical margins were involved in 10 (47.6%) patients. Resection of contiguous organs was required in 15 (71.4%) to achieve gross surgical margins. Eleven of 21 (52%) patients had tumor recurrence. Median disease-free survival was 19 months and the overall 3- and 5-year survival rates were 87% and 49%, respectively.
Our study based on a Korean population from a single tertiary medical center evaluated 19 patients who underwent RPLS treatment. Histopathologic subtypes included 26.3% WD, 10.5% dedifferentiated, and 15.8% myxoid/RC. The remaining 47.4% were mixed-type, accounting for a considerably high proportion of cases. Two cases were composed of WD and dedifferentiated. This may reflect the popular theory that dedifferentiated LPS is a transition from WD LPS to a nonlipogenic sarcoma [29,30]. Even without these two cases, 36.8% were "true" mixed-type RPLS. Mixed-type RPLS is a rare subtype [31,32]. There were no reports of mixed-type RPLS in the other studies we reviewed [4-6]. De Vreeze et al. [33] recently reported a radiological, histopathological, and molecular biological analysis of mixed-type LPS. In that study, 9 patients with lower-extremity LPS presented with a mixed morphology (WD and myxoid). However, immunohistochemical analysis of MDM2 and CDK4 confirmed 4 patients with WD and 5 patients with myxoid.
In our study, the overall survival rate was 84.2% (16 of 19 patients) during a mean follow-up of 66.8 months. The 3- and 5-year survival rates were 86.9%, and the 10-year survival rate was 69.5%. This is comparable to previous RPLS studies reporting an overall survival rate of 52 to 74% during a mean follow-up of 26 to 60 months [4,5,7]. Singer et al. [4] reported 3- and 5-year survival rates of 73% and 60%, respectively, and Milone et al. [7] reported a 5-year survival rate of 85.7% when complete resection was achieved.
In our study, recurrence after initial surgery occurred in 9 of 17 patients (52.9%) after a mean of 93 months. The disease-free rate of primary RPLS at 3 and 5 years was 66.1% and 47.0%, respectively. The overall mean interval between operations was 47.7 months. This was similar to previous reports of recurrence rates of 41.4 to 55.6% with a disease-free period of 20 to 45 months [4,5,7]. Singer et al. [4] reported a disease-free rate of 52% and 41%, respectively, at the 3- and 5-year follow-ups.
According to the study of Singer et al. [4], local recurrence size and local recurrence growth rate independently influence the development of a second local recurrence. They proposed a "one centimeter per month rule": RPLS with a growth rate lower than 0.9 cm per month on the first recurrence presents with a better disease-specific survival and is associated with improved survival after aggressive resection of the local recurrence [20]. In our study, the mean growth rate of tumors on the first recurrence was 0.34 cm per month. All but one patient had a growth rate less than 0.9 cm per month. This may explain the relatively high survival rate of our study. However, local recurrence size was not a significant prognostic factor for locally recurred RPLS.
Our survival and recurrence rates were higher than those previously reported for Asians by Lee et al. [6]. Their lower survival rate probably owes to the high margin-positive rate of 47.6%, despite an aggressive surgical approach with a contiguous organ resection rate of 71.4%. The recurrence interval had a tendency to shorten as the disease recurred again, from 93 months on first recurrence to 24.3 and 8 months on the second and third recurrences, respectively. The recurrence interval was significantly shorter in recurrent RPLS cases than in primary cases. This finding is consistent with the report by Neuhaus et al.[5].
An interesting fact in our study was the high proportion of mixed-type LPS. The long-term survivors of our study (50%), even with the WD/dedifferentiated variant excluded, presented with various subtypes. In some cases, the primary and recurrent RPLS of the same patient showed different histopathologic subtypes. Mixed-type LPS is a rare entity that has yet to be fully illuminated.
CONCLUSIONS
RPLS is the most common histologic type of retroperitoneal malignant tumors. Many studies have been published on RPLS, and complete resection is the gold standard of treatment, leading to increased survival rates and lower recurrence rates. Even in unresectable cases, partial resection may be beneficial. Whether chemotherapy or radiation therapy is effective is still under debate. Even after complete resection, disease recurrence is common and thus repeated resection is recommended.
Our study reported higher survival rates than reported by other groups. The low tumor growth rate of recurrent RPLS in this study may be attributed to such results. Recurrence rates were higher and the recurrence interval was shorter in recurrent RPLS.
Another interesting result of our study was the high prevalence of the mixed type of RPLS. The cause of this high prevalence and whether it is associated with better prognosis is not known and requires further research.




 XML Download
XML Download