

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The era of prostate-specific antigen (PSA) screening has resulted in an increase in the number of prostate biopsies being performed and as a result an increased detection of prostatic intraepithelial neoplasia (PIN) on microscopic examination [1]. The specific diagnosis of PIN had historically created some debate and uncertainty in terms of its clinical significance and relationship to prostate cancer. However, more recent studies confirm that high-grade PIN (HGPIN) shares a clinical, morphological, and genetic background with prostate cancer. In the current report, we review the recent literature pertaining to this entity and the clinical recommendations once a diagnosis of HGPIN is established.
EPIDEMIOLOGY
PIN, which was initially referred to as "intraductal dysplasia," was first described to be a direct biological precursor to prostatic adenocarcinoma by McNeal and Bostwick [2] in 1986. Although in the initial description of PIN the classification included three different grades of dysplasia, at the present time, only HGPIN is reported by pathologists. This is mostly the result of the poor reproducibility among pathologists of distinguishing between low-grade PIN and benign prostate tissue [1,3]. Numerous studies since the initial description have confirmed HGPIN as an accepted precursor to some prostatic adenocarcinomas, and as such it has become a clinically important finding on prostate biopsy in terms of possessing high predictive value for cancer [4]. The estimated time frame to disease progression after HGPIN findings has been reported to be between 29 and 36 months [5,6]. In addition, an increase in the size and number of HGPIN foci has been associated with both prostate adenocarcinoma and its multifocality [7-13]. HGPIN and carcinoma tend to preferentially involve the peripheral zone of the prostate [8,9], and recently many biomarkers and molecular changes such as TMPRSS2-ERG gene fusion have been described in both entities (as discussed further below) [14,15].
The population incidence of HGPIN seems to parallel that of prostate adenocarcinoma. Previous autopsy studies revealed that HGPIN had a low prevalence in men during their third decade of life (7% in African Americans vs. 8% in Caucasians) and progressively increased with advancing age (91% in African Americans vs. 67% in Caucasians) [16]. Sakr et al. [16,17] also observed a higher prevalence of HGPIN in African Americans than in age-matched Caucasian men, similar to prostate cancer. However, the reported incidence of HGPIN in men participating in PSA screening after needle biopsy varies widely according to different series, ranging from 0 to 25% with a mean incidence of 7.7% [4,10,18,19]. Once again, these diverse findings may be explained by the subjectivity of individual pathologists concerning what constitutes HGPIN and possibly by the technical aspects of tissue preparation [18].
The incidence of HGPIN in Asian men is similar to that in Western men. In a study of Korean men undergoing radical cystoprostatectomy, 21% of the men who had no prostate cancer in the final pathology were actually discovered to have HGPIN. As in studies of other races, HGPIN did not correlate with PSA, tumor volume, stage, grade, surgical margins, or lymphovascular invasion [20]. Han et al. [20] also found that both Western and Korean men have high rates of PIN associated with prostate cancer in prostatectomy specimens. In a study from Singapore consisting of 48 Chinese, 3 Malays, 2 Indians, and 3 other men with isolated HGPIN, 24% of those who underwent repeat biopsies had prostate cancer. The authors also observed that most cases of HGPIN affected only one core (79%), with 18% and 4% of cases affecting two and three cores, respectively [21].
HISTORY AND EVOLUTION OF THE DEFINITION OF HGPIN
Historically, isolated HGPIN on the initial core biopsy was reported to be associated with a very high risk of prostate cancer on the repeat biopsy, up to 80% in some series [5,18,22-24]. In the contemporary era, this risk seems to have decreased to approximately 24%, which is slightly higher than the 19% found after repeat biopsy for a benign diagnosis [5,18]. This decrease in the incidence of cancer following a diagnosis of HGPIN is likely related to the increase in the number of needle core biopsies taken, which has improved the accuracy of the initial biopsy. As one would expect with a pre-malignant lesion, the rate of cancer detection on repeat biopsy has been strongly correlated with an increasing number of cores (≥2) containing HGPIN in the initial biopsy [7,12,13]. As a result, this has led to the recommendation of repeat prostate biopsy within 1 year of such findings. Interestingly, neither the initial PSA level nor PSA velocity at the time of HGPIN discovery correlates with the risk of cancer on repeat biopsy [12,13]. Likewise, digital rectal examination, transrectal ultrasound, and other imaging studies have not been shown to be useful in detecting HGPIN [12,13].
MOLECULAR AND GENETIC ALTERATIONS
More than 50 genetic and molecular abnormalities have been associated with HGPIN. At least 10 of these changes are reported in both HGPIN and prostate cancer [25-33]. In addition, more than 36 genetic and molecular alterations are intermediate between normal prostate and prostate cancer [25]. This has led to multiple studies making the conclusion that "High-grade PIN is the most likely precursor of prostatic adenocarcinoma, according to virtually all available evidence" [10,34,35]. Two excellent reviews that list in great detail the known genetic and molecular changes in HGPIN were published by Bostwick and Qian [25] and Mosquera et al. [33], and readers are encouraged to read them.
The TMPRSS2-ERG gene fusion has been found in 30 to 79% of prostate cancers [36] and is associated with aggressive disease in some studies [37,38] but not in others [39]. This fusion has also been discovered in 16 to 19% of HGPIN lesions in patients with prostate cancer [15,33]. Because the cancer had the same fusion pattern as the HGPIN in all cases, it has been postulated that the HGPIN may be the premalignant lesion from which the cancer arose [33].
Multiple mechanisms leading to the dysregulation of cell proliferation and survival have been observed to be present in HGPIN. For example, overexpression of Prostate Tumor Overexpressed-1 contributes to cell proliferation in prostate cancer. In HGPIN, it was shown to be an independent predictor of prostate cancer on repeat biopsy [40]. In addition, up-regulation of the mammalian target of rapamycin (mTOR) pathway promotes prostate cancer. A protein known as 14-3-3σ, which regulates the mTOR pathway, shows progressively increasing levels of expression from HGPIN through Gleason score 6, Gleason score 7, and high-grade prostate cancer [41]. The RER+ phenotype leads to the inactivation of many tumor suppressor genes. In one study, the RER+ phenotype was found in 4% of non-cancerous prostate tissues, 16% of PIN lesions, and 42% of prostate cancer lesions [27]. The same study found microsatellite instability in 12%, 35%, and 53% of normal, PIN, and cancerous tissues. Fatty acid synthetase (FAS) expression, which is thought to be an early event in malignant transformation, has been shown to be overexpressed in HGPIN and prostate cancer, but no FAS expression was observed in normal tissue [42]. Likewise, P53 mutations were detected in 14% of PIN and 25% of prostate cancer lesions in one study [43]. Bcl-2, a proto-oncogene that inhibits apoptosis, has been expressed in many prostate cancers, and has also been reported by Baltaci et al. [28] to be present in both low-grade PIN and HGPIN after immunohistochemical evaluation.
Abnormalities in chromosomes, chromatin structure, and DNA processing enzymes have also been described in HGPIN. More than half of HGPIN lesions may have chromosomal anomalies, including gains of chromosomes (decreasing order of frequency) 8, 10, 7, 12, and Y [26,29]. One study discovered loss of heterozygosity on chromosome 8p12-21 in 63% of PIN lesions in patients with prostate cancer [26]. Telomerase, which can contribute to cancer cell immortalization, is active is some HGPIN foci [32]. DNA topoisomerase II-alpha staining by immunohistochemistry is intermediate between benign tissue and prostate cancer [30]. HGPIN also displays epigenetic changes, including hypermethylation [44].
HISTOPATHOLOGIC CHARACTERISTICS
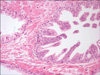
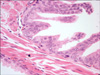
HGPIN is characterized by a proliferation of secretory cells with significant cytologic atypia within the prostate glands and acini. The secretory cells are enlarged with an increased nuclear/cytoplasmic ratio and prominent nucleoli (Fig. 1). The cytoplasm of the HGPIN cells tends to stain positively for α-methylacyl-CoA. Most of these features are shared by invasive prostate cancer [10,25,45]. However, in contrast to prostatic adenocarcinoma in which the basal cells are absent, in HGPIN the basal cell layer is retained although it is often discontinuous on hematoxylin and eosin stain (Fig. 2) [45]. Immunohistochemical staining with antibodies to high molecular weight cytokeratins or nuclear p63 may help in the diagnosis because the presence of basal cells is easily demonstrated [10,19].
DOES HGPIN PREDICT PROSTATE CANCER ON REPEAT BIOPSY?
Perhaps the most important question about HGPIN is whether its presence signals a higher risk of developing prostate cancer. For men who do not have cancer on prostate biopsy, are those with HGPIN more likely to be diagnosed with prostate cancer in the future than are those with only benign tissue on the initial biopsy? Historically, the answer was "yes." Prior to the era of intense PSA screening and before the implementation of extended prostate biopsy schemes, HGPIN indicated up to an 80% probability of finding prostate cancer on additional biopsies [22]. At the time, it was astutely observed that "The finding of high-grade PIN on needle biopsy often represents a sampling problem with carcinoma nearby" [22]. Because the number of cores routinely sampled at prostate biopsy has increased, the predictive value of HGPIN for prostate cancer has decreased. In studies published before 2000, the prostate cancer detection rate was 36% on follow-up biopsy, but after 2000, this rate dropped to 21% [47]. Another review of studies published after 2000 found the risk of cancer on subsequent biopsy to be 5% lower for patients with HGPIN than for those with benign disease [18]. Two reviews by Bostwick et al. tabulate the details of multiple studies of the cancer detection rate in patients with HGPIN [25,48].
Several studies have shown that taking at least 8 cores on the initial biopsy leads to a low prostate cancer detection rate on repeat biopsy [49,50]. In men diagnosed with HGPIN during initial extended biopsies (at least 10 cores), taking more cores (at least 20) on repeat biopsies was an independent predictor of prostate cancer detection, after multivariate adjustment for age, PSA, days from initial biopsy, DRE status, and multifocal PIN [51]. In-office 24-core saturation biopsy detects prostate cancer in 18% of men with HGPIN detected on a prior biopsy [52].
Multifocal HGPIN on biopsy predicts a higher rate of prostate cancer on repeat biopsy than does a single focus of HGPIN [13,53,54]. The evidence for this finding has been noted in multiple studies, and multifocality has been established as a consistent predictor. Roscigno et al. [53] incorporated multifocality along with PSA level, age, and ≤ 12-core initial biopsy into a nomogram that was 72% accurate in predicting prostate cancer on repeat biopsy. The current data on the prognostic value of single versus multiple cores of HGPIN are summarized in Table 1. Studies on the rate of subsequent cancer diagnosis in men with HGPIN on limited vs. extended vs. saturation biopsy schemes are summarized in Table 2.
TREATMENT RECOMMENDATIONS
The management of patients with HGPIN depends largely on the interpretation of the data presented above. Guidelines from the European Association of Urology state that "HGPIN as an isolated finding is no longer considered an indication for re-biopsy" unless it occurs multifocally [55]. The National Comprehensive Cancer Network acknowledges the need for an extended biopsy scheme in their guidelines that "recommend a repeat biopsy using an extended pattern including transition zone if non-focal HGPIN is found on a sextant biopsy. If extended biopsies were used initially, a delayed strategy (re-biopsy 1 year after initial biopsy) may be considered" [56].
Despite the similar rates of cancer detection in men with monofocal HGPIN and benign biopsies, some sources continue to recommend repeat biopsy at 1 year for such findings [48]. However, we feel that based on the currently available data, men with monofocal HGPIN do not need a scheduled repeat biopsy, but that the decision for repeat biopsy should be based on standard clinical factors (rising PSA, new nodule on DRE, etc). Others also espouse this approach [18,57]. We also feel that the evidence supports repeat biopsy for multifocal HGPIN and for patients who had fewer than 10 cores taken on the initial biopsy. Given the low correlation between HGPIN and prostate cancer, nearly all sources recommend against radical prostatectomy, radiation, or androgen deprivation therapy for isolated HGPIN.
A number of studies have investigated possible therapies to lower the incidence of HGPIN or to decrease the rate of progression from HGPIN to prostate cancer [48]. The Prostate Cancer Prevention Trial demonstrated that 7 years of treatment with daily finasteride decreased the incidence of HGPIN from 7.1 to 6.0% [58]. Similarly, in the REDUCE trial, dutasteride reduced the incidence of HGPIN from 6.0 to 3.7% [59]. Green tea catechins for 1 year in men with HGPIN reduced the incidence of cancer from 30 to 3% [60]. Soy, vitamin E, and selenium did not slow the rate of progression of HGPIN to prostate cancer in a randomized double-blind trial in 303 men [61]. We do not routinely recommend any of these therapies to men with HGPIN.
CONCLUSIONS
HGPIN is a relatively common finding in prostate biopsies, and it has been established as a precursor to prostate adenocarcinoma. Its predictive value of increased risk of developing future cancer is low when identified in isolation or in low volume. However, a repeat biopsy should be strongly considered if the initial biopsy contains less than 10 cores or if the HGPIN is present in large volume and within multiple cores.


 XML Download
XML Download