

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Benign prostatic hyperplasia (BPH) is a progressive disease that can cause acute urinary retention (AUR) and that leads to BPH-related surgery [1-3]. At present, alpha-adrenergic receptor blockers (α-blockers) and 5-alpha-reductase inhibitors (5-ARIs) are used in the medical therapy of BPH. Most doctors in the 1990s, however, preferred α-blocker monotherapy to the combination therapy of α-blockers and 5-ARIs. This preference was based on the results of many studies, including a Veterans Affairs Cooperative study and a Prospective European Doxazosin and Combination Therapy Trial study, that reported no significant difference in short-term effects on the treatment of BPH between α-blocker monotherapy and the combination therapy with an α-blocker and 5-ARI [4,5]. In contrast to these reports, the Medical Therapy of Prostatic Symptoms (MTOPS) study reported that during 4.5 years of follow-up, the progression of BPH, the worsening of symptoms, and BPH-related surgeries decreased more in the doxazosin and finasteride combination group than in the doxazosin or finasteride monotherapy group [6]. Furthermore, Kim et al. [7] reported that the incidences of AUR and BPH-related surgeries in a combination therapy group were significantly decreased for 6 to 8 years.
In the present study, the authors analyzed the long-term effects of α-blocker monotherapy and combination therapy with an α-blocker and 5-ARI in actual clinical studies for over 10 years and examined the incidences of AUR and BPH-related surgeries by prostate volume (PV) and prostate-specific antigen (PSA) level.
MATERIALS AND METHODS
This study investigated the medical records of 620 BPH patients who received medical therapy for at least 1 year between January 1989 and July 2010, retrospectively. This study excluded patients who were under 40 years of age; those with an International Prostate Symptom Score (IPSS) of 7 or lower; those whose maximal urinary flow rate (Qmax) was 15 ml/s or higher; patients who had received medical treatment for BPH previously; patients who had received combination medication with anticholinergics; patients who had undergone BPH-related surgery, urinary bladder surgery, urethroplasty, or diathermy; and patients who had lower urinary tract symptoms (LUTS) due to causes other than BPH. Also excluded were patients who had AUR or who had undergone a BPH-related surgery within 12 months after beginning medical treatment and patients who were confirmed to have prostate cancer and BPH simultaneously.
The follow-up period of this study was determined by the AUR onset date, BPH-related surgery date, or last visit date in the medical records. For subjects who were not followed up, information on the continuation of medical treatment, AUR, or BPH-related surgery was collected via mail or phone surveys.
The patients were divided into the α-blocker group, who received α-blocker monotherapy, and the combination group, who received combination therapy of α-blocker and 5-ARI. The incidences of AUR and BPH-related surgeries were compared between these two groups and also between patients who were classified by PV and serum PSA level.
To calculate PV, transrectal ultrasonography was performed. The anteroposterior (H) and transverse (W) lengths were measured from the longest transverse image of the prostate. The horizontal length from the proximal to the distal parts of the prostate in the midline sagittal scan was regarded as the longitudinal (L) length. To calculate PV, the following equation was used: PV=π/6x HxWxL.
To stratify PSA levels and PV, their relationships with
AUR and BPH-related surgeries were examined by using
receiver operating characteristic (ROC) curves.
RESULTS
Of the 620 patients, 368 belonged to the α-blocker group and 252 to the combination group. In the α-blocker and combination groups, respectively, the mean age was 64.2 years (range, 29 to 91 years) and 64.8 years (range, 40 to 89 years) (p=0.470), and the average follow-up period was 108.6 months (range, 12 to 216 months) and 113.1 months (range, 12 to 170 months) (p=0.206). The PSA levels at the first visit of the α-blocker group and the combination group were 2.2 ng/ml and 2.9 ng/ml (p=0.082), respectively, and the PVs were 37.5 ml and 42.9 ml (p=0.064), respectively.
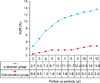
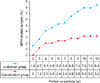
AUR developed in 9.2% (57/620) of the total group: 13.6% (50/368) in the α-blocker group and 2.8% (7/252) in the combination group. Thus, the hazard ratio of the combination group was lower by 79.4% than that of the α-blocker group (p<0.001) (Table 1, Fig. 1). The incidence of BPH-related surgeries was 8.4% (31/368) for the α-blocker group and 3.2% (8/252) for the combination group. Thus, the hazard ratio of the combination group was 61.9% lower than that of the α-blocker group (p=0.008) (Fig. 2).
The incidence of BPH-related surgery was 5.4% for the α-blocker group and 2.4% for the combination group for up to 7 years of follow-up and the difference was not significant. For longer periods of follow-up, however, the incidence of BPH-related surgery was significantly lower in the combination group. The incidence of AUR was significantly lower in the combination group for follow-up periods of 2 years or longer.
The cutoff level of PSA and PV for the hazards of AUR and BPH-related surgery were 2.0 ng/ml and 35 ml, respectively. When the PSA level was higher than 2.0 ng/ml, the incidence of AUR in the α-blocker and combination groups was 24.2% (37/153) and 3.8% (5/133), respectively; when the PV was higher than 35 ml, the incidence of AUR was 27.0% (38/141) and 4.0% (6/150), respectively (p<0.001). When the PSA level was higher than 2.0 ng/ml, the incidence of BPH-related surgery in the α-blocker and combination groups was 17.0% (26/153) and 3.8% (5/133), respectively; when the PV was higher than 35 ml, the incidence of BPH-related surgery was 20.6% (29/141) and 4.7% (7/150), respectively (p<0.001).
Of the 39 patients who underwent BPH-related surgeries, 10 received surgeries due to AUR, and the other 29 received surgeries due to insufficient efficacy of drug treatment.
DISCUSSION
BPH can cause various complications, such as AUR, BPH-related surgeries, urinary incontinence, and urinary tract infection [8]. Between α-blockers and 5-ARIs, which are the representative drug treatments for BPH, 5-ARIs are being spotlighted in that they can prevent BPH progression. In the past, however, most studies were skeptical about the effects of combination therapy with α-blockers and 5-ARIs. The Veterans Affairs Cooperative Study showed that α-blocker monotherapy and 5-ARI combination therapy for 12 months decreased the American Urological Association symptom score to 6.1 and 6.2, and increased Qmax to 2.7 and 3.2, with no significant differences between the two therapies [4]. The Prospective European Doxazosin and Combination Therapy Trial reported that α-blocker monotherapy and 5-ARI combination therapy increased Qmax to 3.6 and 3.8 ml/s, and decreased IPSS to 8.3 and 8.5, with no significant differences between the two therapies [5]. These studies, however, compared the effects of drug treatment for short periods of 1 year or less and focused on comparing the changes in LUTS and Qmax rather than on the complications of BPH.
The effects of 5-ARIs were described better in the Proscar Long-Term Efficacy and Safety Study [2]. This study used finasteride for 4 years, which decreased PV by 18% compared with the placebo group and decreased the incidences of AUR and BPH-related surgeries to 57% and 55%, respectively. Later, the MTOPS study also reported the effects of treatments with α-blocker and 5-ARI for 4.5 years [6]. Compared with that in the doxazosin group, the AUR hazard of the combination group decreased by 75%, and the hazard of BPH-related surgeries decreased by 64% and 67% in the finasteride monotherapy group and the combination therapy group, respectively. The PV increased by 24% in the placebo group and the doxazosin group but decreased by 13% and 16% in the finasteride group and the combination group, respectively.
AUR is not only a serious complication of BPH, but also an important indication for BPH-related surgery. Among the many causes of AUR, BPH accounts for 50% [9]. The PSA level in the serum has shown a close correlation with PV [10]. Roehrborn et al. [11] reported that the risk of AUR in patients whose PSA level was 3.4 ng/ml or higher was 4 times that of patients whose PSA level was 1.2 ng/ml or lower. Furthermore, they reported that the risk of AUR in the patients whose PV was 57 g or higher was 3.5 times that of the patients whose PV was 34 g or lower. Jacobsen et al. [12] also reported that when PV exceeded 30 g, the AUR incidence increased at least 3 times. The European Association of Urology Guidelines strongly recommended drug treatment with finasteride for patients who have BPH and serious LUTS and whose PV is greater than 40 g. Bartch et al. [13] suggested that the treatment with 5-ARI would prevent the progress of potential BPH for patients whose serum PSA level is 1.5 ng/ml or higher or whose PV is 30 g or greater. To determine the effect of the treatment method, Kaplan et al. [14] divided patients into three groups (PV smaller than 25 g, 25 to 40 g, or greater than 40 g) for the results of the MTOPS study. The hazard of BPH progression of the group whose PV was smaller than 25 g did not significantly change between the combination group and the doxazosin or finasteride group; however, in the group whose PV was greater than 25 g, the hazard of BPH progression of the combination group decreased compared with that of the doxazosin or finasteride group. Furthermore, the incidence of invasive surgeries in the combination group decreased by 70% compared with the doxazosin group.
A recent CombAT study set the cutoff level for patients with a high hazard of disease progression as a serum PSA value of 1.5 g/l or higher and a PV of 30 ml or greater [15]. A 4-year study with these patients found that the incidence of BPH progression (IPSS score 4 or higher, AUR, incontinence, relapsing urinary tract infection, or renal inadequacy) was 12.6% in the combination group treated with dutasteride and tamsulosin, 17.8% in the dutasteride group, and 21.5% in the tamsulosin group. In the combination group, the decrease in the hazard associated with prostate progression was statistically significant. Compared with that in the tamsulosin group, the AUR hazard, BPH-related surgeries, and IPSS score of the combination group decreased by 67.8%, 70.6%, and 41.3%, respectively [16].
The study by Lee et al. [17] that was conducted at 5 medical centers in Korea compared an α-blocker monotherapy group and a combination therapy group according to PV, PSA, IPSS, and Qmax. During the 4-year follow-up, the IPSS score of the monotherapy group decreased by 6.1, but that of the combination group decreased by 11.5, which was an improved result.
The present study compared an α-blocker group with a combination group: the AUR incidence was 13.6% and 2.8%, respectively, and the incidence of BPH-related surgeries was 8.4% and 3.2%, respectively. The authors did not find significant differences in the length of AUR incidence between the two groups of patients whose PV was 35 g or lower and serum PSA level was 2.0 ng/ml or lower. Compared with that in the α-blocker group, the AUR incidence in the combination group decreased by 85.2% and 84.3% in patients whose PV exceeded 35 g and whose serum PSA level exceeded 2.0 ng/ml, respectively, and the incidence of BPH-related surgeries decreased by 77.2% and 77.6%, respectively.
The present study was meaningful because it was a long-term study of 10 years of actual clinical data rather than a prospective random contrast study. The incidences of AUR and BPH-related surgeries in the BPH patients who received combination therapy with 5-ARI were significantly lower than those in the patients who received α-blocker monotherapy. These results are similar to those of previous studies and show that combination therapy with 5-ARI is helpful even with long-term treatment of 10 years.
The data of our study, including PSA change, prostate size change, IPSS change, residual urine change, and flow rate change, are not enough because the study was retrospective. Thus, our study has limitations concerning absolute assessment. Therefore, more extensive research is believed to be necessary in the future.
CONCLUSIONS
With the use of actual clinical data, the present study found that the combination group that used an α-blocker and a 5-ARI for a long period of 10 years had a decreased hazard of BPH progression, such as AUR and BPH-related surgeries, compared with the α-blocker monotherapy group. Furthermore, in patients whose PV and serum PSA level exceeded 35 g and 2.0 ng/ml, respectively, combination therapy was more effective than monotherapy in decreasing the incidences of AUR and BPH-related surgeries.

 XML Download
XML Download