

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Lower urinary tract symptoms (LUTS) are problematic in daily life and lower the quality of life in affected people. Benign prostatic hyperplasia (BPH) is a common cause of LUTS, and, as the average male life expectancy continues to increase, the number of males suffering from voiding difficulty secondary to BPH will increase accordingly [1]. As males age, their probability of developing LUTS, for which BPH is the most common cause, increases [2]. Treatment of LUTS includes watchful waiting, pharmacotherapy using α1-adrenergic receptor (AR) antagonists and 5α-reductase inhibitors in moderate to mild cases, and surgical therapy such as transurethral resection of the prostate for severe cases [3,4]. In terms of medical therapy, the use of α1-AR antagonists is the recommended treatment [5]. However, α1-AR antagonists act not only in the lower urinary tract, but also in other tissues such as the vasculature, and cause cardiovascular side effects [6,7]. Tamsulosin, a highly selective α1A-AR antagonist that is currently used, does not significantly decrease systolic and diastolic pressure [8].
Harnal D (astellas pharma Korea Inc., Seoul, Korea) was the original brand name of tamsulosin in Korea, and it was considered a reasonable clinical recommendation for patients with BPH-associated LUTS. The objectives of this study were to verify that Sulosin D (Pacificpharma Co., Seoul, Korea), the generic version of tamsulosin, is not inferior to Harnal D in patients with BPH. Our comparison was based on the efficacy and safety results of a dose-finding study conducted in Korean patients [9].
MATERIALS AND METHODS
1. Participants
Male patients aged ≥40 years and <80 years with LUTS were recruited from four sites in Korea. The eligibility criteria included LUTS for at least 6 months, a total score of at least 12 on the International Prostate Symptom Score (IPSS), and a voluntary signature on informed consent forms. The institutional review board at each of the participating clinical centers approved the study, and all the men provided written informed consent.
The exclusion criteria included suspicious hypersensitivity to α-AR antagonists; a disease causing LUTS (urinary tract stone, urethral stricture, urinary tract infection, primary renal disease, neurogenic bladder, prostatitis); a history of prostate cancer, bladder cancer, previous prostate surgery, urethral reconstruction, transurethral resection of the prostate, or hyperthermia treatment; serum PSA ≥4 ng/ml (a patient whose PSA was ≥4 ng/ml and <10 ng/ml with no malignancy as confirmed by prostate biopsy could be included within 1 year); use of α-AR antagonists or anticholinergics in the previous 2 weeks; medicated with 5α-reductase inhibitors (a patient taking a medication at a stable dose before 12 weeks could be included); medicated with vasopressin or desmopressin (a patient taking these medications at a stable dose before 4 weeks could be included); medicated with SSRI or antipsychotic drugs (a patient taking a medication at a stable dose before 12 weeks could be included); a post-void residual (PVR) urine volume of >150 ml; known moderate cardiovascular disease; orthostatic hypotension; hypotension; known geriatric Alzheimer's disease; or participation in another clinical trial within 4 weeks.
2. Interventions
The typical dose of tamsulosin recommended in Korea is 0.2 mg/day, and this regimen was adopted in this study. We randomly assigned participants at a 1:1 ratio to receive 0.2 mg of Sulosin D or 0.2 mg Harnal D once daily for 8 weeks. A permuted-block randomization procedure with randomly assigned block sizes of four and six was used. There were four clinic visits during which data for the primary and secondary outcome measures were collected. Visit 1 involved screening and collection of baseline data, visit 2 involved randomization and baseline data, visit 3 was the 4-week evaluation, and visit 4 was the 8-week evaluation of the primary endpoint. Adverse events data were collected on visits 3 and 4.
3. Outcomes
The primary endpoint for efficacy was a comparison of the change in IPSS from baseline in the experimental groups with that in the control group. The secondary endpoints were changes in maximal uroflowmetry (Qmax), post-voiding residual (PVR), and quality-of-life (QoL) from baseline. The changes in IPSS subscores were also compared. The patient's perception of benefit and global response assessment were compared. Comparisons of efficacy parameters within groups at the endpoint and at baseline were conducted by using RMANOVA. Comparisons of efficacy parameters between groups were conducted by using ANCOVA.
The difference in IPSS change between the two groups from baseline to 8 weeks was calculated. The non-inferiority margin of Δ was set at -2.4. In other words, non-inferiority is indicated if the lower limit of a one-sided 95% confidence interval for the difference of the change in the IPSS falls above this cutoff. The estimated IPSS difference score of -4.8 was based on previous studies of the efficacy of tamsulosin in Asian BPH patients [10]. The number of patients required to verify the non-inferiority of Sulosin D compared with Harnal D with a one-sided statistical significance level of 5% and a power of 80% was calculated to be 52 patients per group (using the formula,  ). We anticipated that about 15% of enrolled patients would be ineligible. Therefore, 122 patients (61 per study group) were recruited. All results are presented as means±standard deviations.
). We anticipated that about 15% of enrolled patients would be ineligible. Therefore, 122 patients (61 per study group) were recruited. All results are presented as means±standard deviations.
). We anticipated that about 15% of enrolled patients would be ineligible. Therefore, 122 patients (61 per study group) were recruited. All results are presented as means±standard deviations.RESULTS
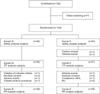
Ultimately, 123 of the 130 men who agreed to participate at the beginning of the screening phase were eligible. Efficacy variables were analyzed on an intent-to-treat basis. A flow diagram of patient allocation is depicted in Fig. 1. The baseline characteristics of each group are presented in Table 1. There were no significant differences between the two groups except in QoL and the storage sum of the IPSS. The mean IPSS was slightly high in the Sulosin D group, but the difference was not significant (18.87±5.62 vs. 17.16±5.22, p=0.1179). Cardiovascular disease and gastrointestinal disease, respectively, were the first and second most commonly reported concomitant diseases in both groups.
The mean changes in primary outcomes at 8 weeks from baseline are summarized in Table 2. After 8 weeks of treatment, patients in the two groups exhibited a significant reduction in IPSS (Sulosin D, -4.97 and Harnal D, -4.03; p<0.0001 for each intra-group comparison). The mean changes in IPSS at 8 weeks were not significantly different between the Sulosin D and Harnal D groups (p=0.9042).
The mean difference in IPSS change over the 8-week treatment period between the two groups was 0.93±6.11 (Harnal D-Sulosin D) in the intent-to-treat cohort, with the 90% confidence interval ranging from -0.91 to 2.77. The lower 90% confidence limit was greater than the prescribed Δ(-2.4) margin. Thus, the non-inferiority of Sulosin D to Harnal D with respect to IPSS improvement was confirmed.
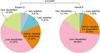
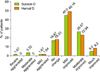
Significant improvements in IPSS subscores and QoL were observed by the end of treatment in both the Sulosin D and Harnal D groups, with the exception of frequency and urgency in the Harnal D group (p=0.1825 and 0.2115, respectively). None of the changes in subscores at 8 weeks were significantly different between the two groups. Moreover, Qmax and PVR were not significantly different (Table 3). The patient perception of benefit after treatment was significantly different in the two groups (Fig. 2). The global response assessment of BPH treatment was not significantly different in the two groups (Fig. 3).
During the treatment periods, adverse events were reported in 23.33% and 34.92% of the Sulosin D and Harnal D groups, respectively, but the incidence of adverse events did not differ significantly between the groups (p=0.1580). However, 13.33% and 11.48% of the Sulosin D and Harnal D groups had adverse events that were considered by the investigator as possibly or probably related to medication.
Only one (1.67%) and two (3.23%) patients in the Sulosin D and Harnal D groups, respectively, withdrew from the study due to adverse events. Almost all of these adverse events resolved without the discontinuation of treatment. There were two patients in each group who discontinued treatment. There were no moderate or severe adverse events in either group. The most common adverse event was dizziness (9.09% with Sulosin D vs. 5.88% with Harnal D). On the basis of the logistic regression analysis, we found that previous medication history and concomitant medication were significantly associated with adverse events (p=0.0442 and p=0.0375, respectively). Prostate size, treatment group, age, and serum PSA were not associated with the occurrence of adverse events.
The mean change in systolic blood pressure from baseline to the end of treatment did not differ significantly between the two groups (Sulosin D, 1.31±12.30 vs. Harnal D, -1.70±11.79, p=0.1738). The change in diastolic pressure was significantly higher in the Harnal D group (Sulosin D, 1.44±8.77 vs. Harnal D, -1.80±6.71; p= 0.0251). There was a significant increase in the pulse rate in the Harnal D group (baseline, 69.33±10.61 vs. 8 weeks 73.54±9.64; p=0.0002), but there was no significant difference between the two groups (Sulosin D, 1.92±10.38 vs. Harnal D, 4.21±8.45; p=0.1853).
DISCUSSION
The present study showed that Sulosin D was not inferior to Harnal D in patients with LUTS symptoms associated with BPH. The changes in total IPSS, QoL, IPSS subscores, Qmax, and PVR after treatment were all comparable between the groups. The within-group improvements in total IPSS score were highly statistically significant (both p-values <0.0001) for the Sulosin D and Harnal D groups. Significant improvements within groups were similar between the groups (p=0.8644). Moreover, the change in total IPSS score in both groups was greater than 4 points, which can be considered perceptible improvement [11]. At baseline, two parameters were statistically different between the two groups: QoL and the storage sum of the IPSS. Because of these parameters, we compared the primary endpoint and secondary endpoints by both the changes in score and those in reduction percentages, both within groups and between groups for each comparison.
Abnormal ejaculation occurred with a greater incidence during tamsulosin 0.4 mg treatment than with placebo. The incidence of abnormal ejaculation with tamsulosin was around 5% to 11% in the US studies [12]. In our study, the abnormal ejaculation rates were 3% and 1.6% in the Sulosin D and Harnal D groups. The abnormal ejaculation rate in our study was less than that of the US studies.
In the patient's perception of benefit, there was a statistically significant difference between the two groups. However, in the global response assessment of treatment of BPH, there were no significant differences between the two groups, and more than half of the subjects answered that they were improved compared with before treatment.
A bioequivalence test has been required since 1989 when generic drugs were approved by the Korea Food and Drug Administration (KFDA) [13]. A bioequivalence study provides important information to ensure the availability of safe and effective medicines to patients. The bioequivalence measure is frequently expressed in terms of systemic exposure measures, such as the area under the plasma concentration-time curve and maximum concentration. Bioequivalence assesses the relative bioavailability of two drug products and focuses on comparative drug product performance [14]. This is established in small bioequivalence studies, which are single-dose crossover studies in healthy subjects comparing peak concentration and total drug exposure during treatment with either reference or generic test formulations [15]. For generic approval, the distributions of the ratio of peak concentrations and concentrations measured over time for a reference compared with the test formulation must be between 80% and 125%. However, there is no evidence that bioequivalence translates to equality in terms of clinical efficacy.
More than 140 generic BPH drug formulations have been approved through the KFDA. Generics account for about 39% of BPH medications in Korea. In terms of pharmaceutical costs, generics account for about 37% of BPH medication costs. In Korea, generic drug costs are 80% of branded drug costs. If bioequivalence indicates equality with respect to clinical efficacy, clinicians will consider using generic drugs. As mentioned earlier, all generics have not been proven to be equivalent to the original brand drugs.
A limitation of our study was that it did not include a placebo group. To confirm the efficacy of a generic, a study should determine whether it is superior to placebo and not inferior to the original drug. This hypothesis was the best for evaluating the efficacy of the Sulosin D, but our study did not have a placebo group.
There has not been an equivalence study or a non-inferiority clinical trial for BPH medication. This study may be the first clinical trial to assess the non-inferiority of a generic BPH medication compared with the original drug. If other generic BPH drugs demonstrate equality or non-inferiority, more urologists will prescribe generics, which is likely to result in a decrease in pharmaceutical costs.



 XML Download
XML Download