

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
With the increase in life expectancy, there has been a growing interest in age-related conditions such as lower urinary tract symptoms/benign prostatic hyperplasia (LUTS/BPH) and sexual dysfunction in the past few years. Because LUTS/BPH and sexual dysfunction are highly prevalent conditions that have substantially adverse impacts on quality of life (QoL) in elderly men, many studies have evaluated a causal relationship between LUTS/BPH and sexual function, although such a relationship remains controversial [1-6].
Because of the possible association between LUTS/BPH and sexual function, several studies have evaluated the influence of various treatments for LUTS/BPH on sexual function [6-12]. The previous studies on transurethral resection of the prostate (TURP), the reference standard of surgical treatment for LUTS/BPH, have shown mixed results in terms of postoperative sexual function [6-9,12]. Recent studies that specifically evaluated sexual function following photoselective vaporization of the prostate (PVP) reported improvements or maintenance of sexual function after surgery [10,13,14]. Also, recent studies on holmium laser enucleation of the prostate (HoLEP), an attractive alternative to TURP, have shown no significant changes in overall sexual function at one or two time points of follow-up after surgery [11,15].
To date, however, data are sparse on the serial changes in sexual function in the short-term period following HoLEP as assessed by use of validated tools. We therefore aimed to evaluate the serial changes in sexual function in the short-term period after HoLEP for LUTS/BPH by use of the International Index of Erectile Function (IIEF) and to investigate whether a change in each domain of the IIEF was associated with improvement of micturition.
MATERIALS AND METHODS
1. Study design
Approval for this study was provided by the Internal Review Board of our Hospital. Of 95 potent men who underwent HoLEP for LUTS/BPH refractory to medical therapy with an alpha-blocker between July 2008 and April 2009 by a single surgeon, complete 12-month follow-up data on the IIEF were available for 53 patients. After excluding patients 1) who had a history of previous prostatic surgery, 2) with urethral stricture or neurogenic bladder or prostatic malignancy, or 3) who did not have sexual intercourse within 4 weeks before surgery or each follow-up visit, a total of 38 patients were eligible for analysis.
All patients underwent a baseline evaluation with the IIEF, transrectal ultrasonography (TRUS), and multichannel video urodynamic study (MMS UD-2000; Medical Measurement System, Ennschede, The Netherlands) in addition to a general standard evaluation for LUTS/BPH including history, physical examination including digital rectal examination, International Prostate Symptom Score (IPSS), and serum prostate-specific antigen (PSA). After HoLEP, surgical outcomes of the treatment for LUTS/BPH were assessed at 1, 3, 6, and 12 months postoperatively by use of the IIEF, IPSS, uroflowmetry, and post-void residual urine volume (PVR). Retrograde ejaculation was documented by an urologist on the basis of the medical history at the follow-up visit.
2. Intervention
All surgical procedures were performed in a routine manner as previously described in detail [16]. Briefly, the first step was the exposure of the surgical capsule by incisions at the 5 and 7 o'clock positions just above the verumontanum. These incisions were connected to each other in the shape of an inverted "U" by an incision at the 6 o'clock position. The median lobe was then enucleated along the surgical capsule in a retrograde fashion. The surgical capsule in the 12 o'clock position of the apex was exposed through a midline incision, which was extended from the bladder neck to the apex. The incision was then connected from the lateral edge to the 12 o'clock position and retrograde enucleation of the lateral lobes was performed. Morcellation of three enucleated lobes was performed in a routine manner. At the end of surgery, a 20 Fr three-way urethral Foley catheter was placed, and the balloon was inflated with 30 ml of saline.
3. Statistical analysis
Change in serial sexual function was evaluated by comparing the total IIEF score as well as each individual domain score between baseline and each follow-up after surgery by use of the paired t-test. To systemically monitor changes in erectile function over time after surgery, the severity of erectile dysfunction (ED) in the patients was stratified into the following five categories according to the erectile function (EF) domain score of the IIEF: no ED (EF domain score 26 to 30), mild ED (EF score, 22 to 25), mild to moderate ED (EF score, 17 to 21), moderate ED (EF score, 11 to 16), and severe ED (EF score, 6 to 10) [17]. The proportional changes in each category were analyzed throughout the follow-up period after HoLEP. We used the Pearson correlation test to assess the significance of correlations between change in each IIEF domain score and that in each variable of IPSS or uroflowmetry. A 5% level of significance was used for all statistical testing, and all statistical tests were two-sided. SPSS ver. 17.0 (SPSS Inc., Chicago, IL, USA) was used for the data analysis.
RESULTS
1. Baseline characteristics and perioperative variables
The baseline characteristics and perioperative variables are shown in Table 1. Mean age and body mass index of all eligible patients were 64.5±6.2 years and 24.2±2.6 kg/m2, respectively. Mean serum PSA, total prostate volume, and transitional zone volume were 3.1±3.2 ng/ml, 48.8±18.8 ml, and 24.2±16.1 ml, respectively. Seven (18.4%) patients received medication with 5-alpha reductase inhibitors before surgery. There were no major intraoperative complications such as severe bleeding requiring blood transfusion, but capsular perforation, bladder mucosal injury, de novo stress urinary incontinence, and de novo urgency urinary incontinence were observed in 1, 4, 1, and 6 cases, respectively. Twenty (52%) patients complained of retrograde ejaculation after the surgery.
2. Serial changes in micturition parameters and sexual function after HoLEP
Table 2 summarizes the subjective and objective outcomes after HoLEP. As expected, both subtotal voiding symptom scores and total IPSS scores were significantly reduced compared with baseline starting from 1 month after the HoLEP procedure, which was associated with a significant improvement in the QoL index. In contrast, the subtotal storage symptom scores were significantly reduced compared with baseline starting from 3 months after surgery. All IIEF domain scores showed a slight decrease at 1, 3, and 6 months after surgery compared with baseline, although these changes were not statistically significant except for the orgasmic function and overall sexual satisfaction domain scores at 6 months after HoLEP. Also, at 12 months after HoLEP, all IIEF domain scores except for orgasmic function and overall sexual satisfaction recovered to the baseline or showed a marginal but nonsignificant increase compared with baseline. In contrast, both orgasmic function and overall sexual satisfaction domain scores were still slightly decreased at the 12-month follow-up compared with baseline, but this was not statistically significant. Of the two items that compose the orgasmic function domain, the score of "ejaculation frequency" at 1, 3, and 6 months after HoLEP was significantly decreased compared with baseline (p<0.05). Even at 12 months after surgery, the score of "ejaculation frequency" was still slightly reduced compared with baseline, but this was not statistically significant (p=0.070).
3. Prevalence and severity of ED according to the follow-up period after HoLEP
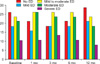
Fig. 1 shows the prevalence and severity of ED according to the follow-up period after HoLEP. The percentages of patients with erectile dysfunction before surgery and at 1, 3, 6, and 12 months after HoLEP were 73.7%, 78.9%, 81.6%, 78.9%, and 71.1%, respectively. The percentages of patients with normal EF or mild ED at 1, 3, and 6 months after surgery were slightly decreased compared with baseline, whereas the percentages of patients with mild-to-moderate or moderate ED were slightly increased, but not significantly so. In contrast, the percentage of patients with normal EF or mild ED at 12 months after surgery was slightly increased compared with baseline, whereas the percentage of patients with moderate or severe ED was slightly decreased, which was not statistically significant.
4. Correlation between changes in micturition and sexual function
We performed the Pearson correlation test to assess whether change in sexual function after HoLEP was associated with improvement in micturition symptoms. There was no significant correlation between improvement in each variable of the IPSS or uroflowmetry and change in each IIEF domain score during the entire period of follow-up after the HoLEP procedure.
DISCUSSION
There are several data in the published literature evaluating the effect of HoLEP for LUTS/BPH on sexual function [11,15,18-21]. However, some studies used nonvalidated tools for evaluation of postoperative sexual function, and even other studies that used validated questionnaires did not analyze serial changes in the individual items or each domain score of the questionnaires in the early postoperative period after HoLEP. To our knowledge, our study is the first to evaluate serial changes in sexual function by use of a validated questionnaire in the short-term, early postoperative period after HoLEP. Thus, our data can extend the current state of knowledge in the area of sexual function after BPH surgery by further exploring the serial changes in sexual function in the early postoperative period after HoLEP. The important findings of our study can be summarized as follows: 1) overall sexual function was slightly deteriorated in the early postoperative period after HoLEP, but recovered to the baseline at 1 year postoperatively; 2) different from other IIEF domain scores, the orgasmic function or overall sexual satisfaction domain score was slightly decreased and this decrease lasted up to 12 months following HoLEP, probably due to ejaculatory problems; 3) there was no significant correlation between improvement of micturition and change in sexual function throughout the follow-up period after HoLEP.
As suggested by our results, sexual function appears to be transiently decreased in the early postoperative period after HoLEP. Uygur et al. [22] showed that ED developed in 5% and 6% of potent patients at 3 months after open prostatectomy or TURP, respectively, but that EF recovered in about half of them at 6 months postoperatively. Also, a previous study by Tscholl et al. [23] using the snap-gauge test at 4 days and 3 months after TURP showed a high rate of ED in the immediate postoperative period, which significantly improved at retesting. A recent study by Choi et al. [24] showed that the EF domain score was decreased at 1 and 3 months after TURP but recovered to the baseline at 6 months after surgery. Thus, the ED seen immediately after BPH surgery may be temporary and due to the neurapraxia induced by thermal injury or emotional stress [15]. This is supported by the result of a study by Zohar et al. [25] showing that patients with LUTS/BPH reportedly tend to be anxious and less satisfied with their sexual life and that the level of anxiety exhibited by the patient is a predictor of potency after prostatectomy. Furthermore, Meng et al. [11] suggested that injury to the urethra could affect patients as pain during erection after HoLEP.
Another interesting finding was that the orgasmic function or overall sexual satisfaction domain score remained slightly decreased throughout the follow-up period after the HoLEP procedure. In the present study, the scores of "ejaculation frequency," one of two items that compose the orgasmic function domain, were decreased throughout the follow-up period after HoLEP compared with baseline, although not significantly so at 12 months after surgery. Therefore, ejaculatory problems may have an adverse effect on orgasmic function or overall sexual satisfaction after HoLEP. This finding is in accordance with the study by Briganti et al. [15] showing a significant deterioration in the mean IIEF orgasmic function domain score after HoLEP and a recent study by Muntener et al. [12] suggesting that the loss of ejaculatory function after TURP is significant and is associated with considerable bother.
The present study did not demonstrate a significant correlation between improvement of micturition and change in sexual function after HoLEP. Although some studies have shown a correlation between LUTS/BPH and sexual dysfunction [2-5,26], the epidemiologic data do not support a causal relationship based on Hill's criteria for causality between the two. Thus, it remains unclear whether sexual dysfunction in older men is causally related to BPH or is merely a consequence of aging [27]. Moreover, the evaluation of sexual function in patients treated with TURP or PVP has been associated with mixed results [6-10,12-14]. Thus, the effect of BPH surgery on sexual function is still controversial. In accordance with our results, most recent studies have demonstrated no significant effect of HoLEP on sexual function after surgery in patients with LUTS/BPH [18-21].
Some limitations of our study warrant consideration. First, the present study is limited by both its retrospective nature and the fact that it was conducted at a single institution and therefore carries with it all the inherent potential issues associated with such studies. Second, the follow-up period was only in the short-term. However, alterations of sexual function more than 1 year after surgery may be significantly attributed to aging and comorbidities rather than the HoLEP procedure. Third, although retrograde ejaculation was queried at every follow-up visit, the IIEF cannot assess this condition completely. Fourth, our population was not large enough to perform an analysis in subgroups such as patients with no or mild ED or to allow for multivariate analysis. However, our data can be used to counsel patients regarding realistic expectations of sexual function after the HoLEP procedure.
CONCLUSIONS
Although HoLEP achieves significant improvements in micturition both subjectively and objectively, overall sexual function decreases slightly in the early postoperative period after but recovers to baseline at 12 months postoperatively. In addition, our data suggest that changes in sexual function after HoLEP are not associated with improvement of micturition symptoms. However, studies with larger cohorts including prospective, multicenter studies are necessary to fully validate these findings.


 XML Download
XML Download