

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Renal neoplasms are composed of heterogeneous groups including clear cell renal cell carcinoma (RCC), papillary RCC, chromophobe RCC, collecting duct carcinoma, oncocytoma, and others. In most cases, these categories are easily differentiated from each other on the basis of histologic features alone. Occasionally, however, there are overlapping morphological characteristics between such tumors as well as histologic heterogeneity within a single tumor. In those cases, it may be difficult to make an accurate subtyping of the tumors.
A diagnostic problem can arise in distinguishing chromophobe RCC from oncocytoma. These two types of tumors have a common origin, distal nephrons, and similar phenotype, so it may be difficult to distinguish these tumors in the practice of diagnostic pathology. Chromophobe RCC and oncocytoma should be distinguished from each other because both tumors have different behaviors and clinical outcomes. Oncocytoma is a benign tumor, whereas chromophobe RCC is a subtype of RCC, namely, malignant. In recent years, several studies have been carried out to find helpful ancillary means to distinguish chromophobe RCC from oncocytoma. However, the results of these studies are inconsistent and still unsatisfactory [1-8].
Caveolin-1, a 24-kd membrane protein, is a major structural and functional protein component of caveolae, endocytic structures of the cell membrane [9,10]. Caveolin-1 plays important roles in membrane traffic, lipid traffic, and signal transduction [9,10]. Several studies have shown that the expression of caveolin-1 is elevated in various types of malignancies such as prostate, breast, colon, esophagus, and urinary bladder cancers [11-14], but the precise roles of caveolin-1 in carcinogenesis are still unclear.
MOC-31 is a kind of cell surface glycoprotein and is expressed in most benign and malignant epithelia. It is known that MOC-31 is useful for distinguishing adenocarcinoma from mesothelioma as well as hepatocellular carcinoma from cholangiocarcinoma and metastatic adenocarcinoma in the liver [15,16].
In this study, we intended to identify whether there were any differences in immunohistochemical reactivity for caveolin-1 and MOC-31 between chromophobe RCC and oncocytoma and to determine whether the expression of these proteins has a benefit as useful immunohistochemical markers in distinguishing the tumors. In addition, clear cell RCC, particularly the granular cell type, may also have a phenotype similar to the previously mentioned two types of tumors and cause a diagnostic problem. Accordingly, we also investigated the immunohistochemical reactivity of clear cell RCC for caveolin-1 and MOC-31 and evaluated the differences among clear cell RCC, chromophobe RCC, and oncocytoma.
MATERIALS AND METHODS
1. Case selection
Twenty-three chromophobe RCCs and 8 oncocytomas were retrieved from the surgical pathology archives between 1997 and 2006 at three institutes. Twenty-five clear cell RCCs, including 10 cases of clear cell type and 15 cases of granular cell type, were also selected from the surgical pathology files of one institute. Those cases were composed of only radical surgical specimens. Two pathologists, one of whom has expertise in genitourinary pathology, reviewed all cases and achieved consensus on classification according to the recommendations of the International Union Against Cancer [17] and the World Health Organization Classification of Tumors [18]. Most tumors were categorized on the basis of light microscopic histology. Electron microscopic examination was performed for 9 cases because they showed obscure and overlapping histologic features on light microscopic, histochemical, and immunohistochemical examinations. Two cases having unclear features despite the electron microscopic examination were excluded from this study. Staging of chromophobe RCC was performed according to the recently updated staging system (7th edition) of the American Joint Committee on Cancer (AJCC) (7th edition) and the Union Internationale Contre le Cancer (UICC) [19]. The clinicopathologic data of all chromophobe RCCs and oncocytomas are summarized in Table 1.
2. Immunohistochemistry
The immunohistochemical staining was performed with the DAKO EnVision Kit (Dako, Denmark) on sections prepared from formalin-fixed and paraffin-embedded specimens that were dewaxed and rehydrated with graded concentrations of alcohol. Endogenous peroxidase was blocked by dipping the sections in 3% aqueous hydrogen peroxide for 10 min, and antigen retrieval was performed with a 10-min microwave treatment in 10 mmol/l citrate buffer, pH 6.0. For immunohistochemical staining of MOC-31, Target Retrieval Solution (Dako, Denmark) was used for antigen retrieval. Diluted primary antibodies for caveolin-1 (1:200, Transduction Laboratories, US) and MOC-31 (1:50, Dako, Denmark) were treated at room temperature for 30 min and 1 h, respectively. After the primary antibody incubation, the sections were incubated with the secondary antibody. The sections were lightly counterstained with hematoxylin.
Immunoreactivity for caveolin-1 and MOC-31 was considered as diffuse positive when 50% or more of the tumor cells were stained, as focal positive when 10% to 49% of the tumor cells were stained, and as negative when less than 10% of the tumor cells were stained. Internal positive controls were endothelial cells and distal tubular epithelial cells for caveolin-1 and MOC-31, respectively.
3. Statistical analysis
Data were analyzed by the Fisher's exact test with SPSS ver. 12.0 (SPSS Inc., Chicago, IL, USA) to evaluate correlation between the tumor types and expression of immunohistochemical stain for caveolin-1 and MOC-31. p-values less than 0.05 were considered statistically significant.
RESULTS
1. Immunoreactivity for Caveolin-1
In normal kidney tissue, expression of caveolin-1 was seen in parietal epithelia of Bowman capsules, endothelial cells, and smooth muscle cells of blood vessels but not in endothelial cells of glomeruli or any other epithelia (Table 2, Fig. 1A).
In chromophobe RCCs, 20 (87%) of 23 cases showed diffuse positivity for caveolin-1. All positive cases showed expression of caveolin-1 in 90% or more of the tumor cells and moderate to strong intensity except for one case that had relatively weak intensity. The pattern of immunohistochemical staining was diffusely cytoplasmic and granular. In most of the cases, the cell membrane was also stained and the staining intensity was stronger in the membrane than in the cytoplasm (Fig. 2A). In the three negative cases, none of the tumor cells expressed caveolin-1.
Oncocytomas showed negative results for caveolin-1 in all eight cases (Fig. 2B). None of the tumor cells expressed caveolin-1 except for one case in which caveolin-1 was expressed in only 5% or less of the tumor cells.
Clear cell RCCs were diffuse positive in 19, focal positive in 2, and negative in 4. The total number of positive cases was 21 (84%) of 25 clear cell RCCs. All 10 cases of the clear cell type were diffuse positive, whereas 9 (60%) of 15 cases of the granular cell type were diffuse positive. There was a slight difference in the pattern of immunohistochemical staining between the clear and granular cell types. All cases of the clear cell type showed dominantly membranous staining without cytoplasmic staining (Fig. 3A), whereas most cases of the granular cell type exhibited a similar staining pattern to that of chromophobe RCC, namely, a diffusely cytoplasmic and granular pattern with focal membranous condensation (Fig. 3B).
2. Immunoreactivity for MOC-31
MOC-31 was positive in distal tubules and collecting ducts of normal kidney tissue but negative in other epithelial and mesenchymal tissues (Table 2, Fig. 1B).
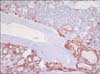
MOC-31 was diffuse positive in 22 (96%) of 23 chromophobe RCCs, showing a strong membranous pattern of immunohistochemical staining (Fig. 4A), and negative in only 1 case.
In oncocytomas, MOC-31 was negative in 6 of 8 cases and diffuse positive in the other 2 cases (25%) (Fig. 4B). Three of the six negative cases expressed MOC-31 in less than 10% of the tumor cells, and the other three cases showed no staining. In the former three cases, MOC-31 was characteristically expressed in the tumor cells showing tubular structures but not solid nests or trabecular structures. In addition, two oncocytomas showing diffuse expression of MOC-31 were composed of predominantly tubular structures, and solid or trabecular structures were only a minor portion. MOC-31 was expressed in such tubular structures rather than in solid or trabecular structures (Fig. 5).
Clear cell RCCs showed relatively variable MOC31 staining results. Clear cell RCCs were diffuse positive for MOC-31 in 12, focal positive in 2, and negative in 11. The total number of positive cases was 14 (56%) of 25 cases. In particular, the granular cell type of clear cell RCC showed less positivity for MOC-31 than did the clear cell type. Only 6 (40%) of 15 cases of the granular cell type were positive for MOC-31. All positive cases showed a membranous staining pattern as for the chromophobe RCCs.
DISCUSSION
Subtypes of renal cell tumors are various and complex. Although each renal cell tumor has unique characteristics, they may occasionally have overlapping histologic features that make it difficult to make a proper diagnosis. One of the most problematic differential diagnoses is to distinguish chromophobe RCC from oncocytoma.
Chromophobe RCC was first described by Thoenes et al in 1985 [20]. Chromophobe RCC consists of tumor cells showing abundant pale cytoplasm with a perinuclear halo and peripheral condensation and hyperchromatic, irregular, wrinkled nuclei. By contrast, oncocytomas have tumor cells showing abundant eosinophilic granular cytoplasm and regular and round nuclei. Both tumors can be distinguished on the basis of these histologic features. However, occasionally, when the tumors show obscure microscopic findings, it can be difficult to make a differential diagnosis. Therefore, many investigators have searched for helpful ancillary means to discriminate these two types of renal tumors.
Electron microscopic examination is an important and useful tool in the differential diagnosis of chromophobe RCC and oncocytoma. However, electron microscopic examination is technically difficult, expensive, and not available in many laboratories. Several studies have suggested that Hale's colloidal iron stain is helpful for the differential diagnosis of chromophobe RCC from oncocytoma [1]. However, Hale's colloidal iron stain is also technically demanding and difficult to interpret, and therefore reproducibility is relatively low [2].
Several studies with various immunohistochemical markers, including kidney-specific cadherin, CK7, EMA, CD10, parvalbumin, RCC, c-KIT, and RON proto-oncogene, have been performed to find useful markers for distinguishing chromophobe RCC from oncocytoma. However, the results of these studies are inconsistent or turned out to be not satisfactory. Accordingly, the use of these markers in differential diagnosis is limited [2-8,21,22].
Caveolin-1 is a major protein component of caveolae, which are endocytic structures of the cell membrane, and is localized to the cytosolic surface of caveolae. Caveolin-1 interacts with both lipids and lipid anchors on proteins; therefore, it has multiple functions in signal transduction, membrane traffic, and intracellular and extracellular lipid transport [9,10]. Expression of this molecule has been studied in various types of tumors, including prostate, breast, colon, esophagus, and urinary bladder cancers [11-14]. However, only a small number of studies have recently reported a relationship between the expression of caveolin-1 and renal neoplasms, including chromophobe RCC and oncocytoma [23-25].
In the present study, caveolin-1 was expressed in 20 (87%) of 23 chromophobe RCCs but in 0 of 8 oncocytomas. All positive cases of chromophobe RCC showed diffuse, moderate to strong staining in 90% or more of tumor cells and cytoplasmic and granular staining with membranous condensation. This clear discrimination enables the use of caveolin-1 for differential diagnosis between chromophobe RCC and oncocytoma (p<0.001).
Carrion et al and Mete et al reported that most oncocytomas express caveolin-1 with a diffuse cytoplasmic staining pattern and that chromophobe RCCs show a relatively decreased expression of caveolin-1 [23,24]. This difference probably originated from the artifact that they did not use a blocking step for endogenous biotin despite using an avidin-biotin peroxidase kit. Endogenous biotin in oncocytomas may cause a false-positive result. Nevertheless, there was a difference in staining pattern between chromophobe RCCs and oncocytomas in their studies. According to them, chromophobe RCCs showed peripheral cytoplasmic staining, whereas oncocytomas showed diffuse cytoplasmic staining. There was an obvious difference in the incidence and staining pattern of caveolin-1 expression between both tumors.
In contrast with these findings, Garcia and Li reported that caveolin-1 was positive in all 21 chromophobe RCCs but was focal positive, with staining in less than 20% of the tumor cells, in only 3 of 26 oncocytomas [25]. This result is consistent with and supports our result.
Occasionally, it may also be difficult to distinguish clear cell RCC, particularly the granular cell type, from chromophobe RCC or oncocytoma in practice. Therefore, our present study also included clear cell RCCs. Twenty-one (84%) of 25 clear cell RCCs were positive for caveolin-1, including 2 focal positive cases. Granular cell type tumors of clear cell RCCs were very similar to chromophobe RCC in staining pattern as well as extent, whereas clear cell type tumors differed from chromophobe RCC, that is, showing membranous staining. On the basis of these results, the granular cell type of clear cell RCC could be differentiated from oncocytoma (p<0.001) but not chromophobe RCC (p=0.466).
MOC-31, a kind of cell surface glycoprotein, is expressed in various benign and malignant epithelia, but its function is still unclear. MOC-31 has been studied for differential diagnosis between hepatocellular carcinoma and cholangiocarcinoma or metastatic adenocarcinoma in the liver or between mesothelioma and adenocarcinoma [15,16]. Studies associated with renal neoplasms have rarely been performed.
In our study, MOC-31 showed diffuse, strong, and membranous staining in 22 (96%) of 23 chromophobe RCCs and diffuse cytoplasmic staining in only 2 (25%) of 8 oncocytomas. The other six cases of oncocytomas were considered to be negative, but three of them expressed MOC31 with cytoplasmic staining in less than 10% of the tumor cells. In these three cases and the diffuse positive two cases of oncocytomas, MOC-31 was predominantly expressed in the tumor cells showing tubular differentiation rather than solid or trabecular structures. This seems to be related to the fact that MOC-31 is expressed in distal tubular cells of normal kidney. Although most oncocytomas do not express MOC-31, some oncocytomas may express MOC-31 if they are differentiated toward tubules and have similar structural features to normal distal tubules. Further molecular analysis is needed to uncover the precise function of MOC-31 in tubular differentiation and tumorigenesis.
According to our result for MOC31 expression, diffuse membranous expression of MOC-31 is a feature of chromophobe RCC rather than of oncocytoma, particularly not showing tubular differentiation (p<0.001). Pan et al showed that 23 (82%) of 28 chromophobe RCCs were positive for MOC-31, whereas all 7 oncocytomas were completely negative [7]. This result is consistent with ours.
Clear cell RCCs expressed MOC-31 in 14 (56%) of 25 cases, including 2 focal positive cases. Considering only the granular cell type, 6 (40%) of 15 cases were positive for MOC-31. As previously mentioned, clear cell RCC had a statistically significant difference in the expression of MOC-31 from chromophobe RCC (p<0.001) but not oncocytoma (p=0.215). For example, if a tumor is negative for MOC-31, it is more likely to be clear cell RCC than chromophobe RCC.
CONCLUSIONS
The results of the present study showed an obvious discrimination between chromophobe RCC and oncocytoma in the expression of caveolin-1 and MOC-31. In other words, these immunohistochemical markers are thought to be considerably useful for distinguishing these tumors. In addition, clear cell RCC also showed a different expression of caveolin-1 and MOC-31 from oncocytoma and chromophobe RCC, respectively. If used together with other known markers such as c-KIT or RCC marker, both caveolin-1 and MOC-31 may be helpful in the differentiation of clear cell RCC from chromophobe RCC or oncocytoma.








 XML Download
XML Download