

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The classification of patients with renal cell carcinoma (RCC) by the level of risk for local recurrence, prognosis, and survival is important for patients and clinicians to consider before surgery so that appropriate treatment and follow-up can be provided. Several anatomical, clinical, histological, and molecular factors have been reported as useful for the prediction of patient prognosis [1]. Since 2001, numerous studies have been performed on a variety of clinical and pathological factors that can be used to determine a more accurate prognosis [2,3]. More recently, the assessment of molecular genetic characteristics has become important for the prediction of tumor-specific survival. Many genes and the associated proteins have been studied for their association with patient prognosis [4]. For example, a recent study from the Mayo Clinic reported that the expression of the B7-H4 protein was detected in a diverse group of malignant tumors including RCC; this protein has been associated with blocking of antitumor mechanisms [5]. B7-H4 was first reported by Chen et al in 2003; it is the ligand of the B7 protein and a suppressor of T cell mediated immunity [6-8]. The B7-H4 protein is overexpressed in lung tumors, breast tumors, and ovarian tumors [9].
RCC has been classified as an immunogenic tumor, with lymphocyte infiltration. On occasion, complete disappearance of metastatic tumors, after the surgical removal of primary tumors, has been observed. However, only 5% to 10% of cases of advanced RCC respond to cytokine-based immunotherapy [10]. The mechanism associated with the ability of renal cancer cells to evade antitumor immunity is unknown and the focus of many current studies.
Currently, due to the increased use of radiological diagnostic techniques and the interest in prevention, the clinical diagnosis of early-stage RCC has increased. The goal of this study was to examine the association of the expression of B7-H4 with the pathological characteristics of RCC, patient prognosis, and disease recurrence in patients with stage T1 RCC.
MATERIALS AND METHODS
1. Materials
Among patients diagnosed with clinical stage T1 RCC who underwent a partial or radical nephrectomy from January 2000 to March 2007, 102 patients were confirmed to have clear cell tumors by the postsurgical pathological evaluation.
2. Clinical and pathological characteristic
Clinical and pathological characteristics were analyzed retrospectively on the basis of information in the patients' medical records. The data collected included age at the time of surgery, gender, tumor size at the time of diagnosis, and the presence or absence of symptoms. Patients with an abdominal lump, abdominal pain, macroscopic hematuria, a varicocele, or weight loss were considered symptomatic at the time of diagnosis. The histological type of tumor, TNM disease stage, nuclear grade, presence or absence of tumor necrosis, and presence or absence of lymphovascular invasion were evaluated.
The definitions of disease progression included local recurrence, lymph-node metastasis, and distant metastasis. However, in this study, no cases of local recurrence were identified.
3. Immunohistochemical staining
Sections 4 µm in thickness were obtained from paraffin-embedded tissues, attached to coated slides, incubated in a 60℃ oven for 1 hour, deparaffinized by repeated treatment with xylene for 5 minutes four times, dehydrated by several steps of alcohol, and washed with distilled water. For antigenic recovery, the slides were soaked in 0.01 M citrate buffer and boiled in a microwave for approximately 10 minutes. Afterwards, the slides were cooled at room temperature for 30 minutes, washed with washing buffer for 3 minutes three times, and reacted in 3% H2O2 solution for 5 minutes to remove intrinsic peroxidase. The slides were washed with wash buffer four times, reacted with the first B7-H4 antibody (Abbiotec 1:500, rabbit polyclonal antibody) overnight at 4℃, washed four times, and reacted with horseradish peroxidase polymer conjugate for 10 minutes. Subsequently, the slides were washed with wash buffer four times, stained with diaminobenzidine, counterstained with hematoxylin, sealed, and examined under the light microscope.
The sporadic expression of B7-H4 protein in the distal convoluted tubules was considered the positive control group. Cases in which expression of the B7-H4 protein was detected in more than 10% of the tumor cells were considered positive, and cases in which expression was less than 10% were considered negative [11]. The results of the staining were interpreted by one pathologist. The tumor cells that were stained reddish brown with B7-H4 antibody were read as positive (Fig. 1).
4. Statistical analysis
The results were divided into groups with and without expression of B7-H4 and clinical and pathological characteristics were analyzed. For the analysis of recurrence-free survival, univariate analysis, Kaplan-Meier, and the logrank tests were performed. For the multivariate survival analysis, Cox's proportional hazard regression model was performed. The factors considered in the analysis included recurrence, age, gender, symptoms at the time of diagnosis, tumor size at the time of diagnosis, pathological disease stage, nuclear grade, lymphovascular invasion, and the expression of B7-H4. SPSS ver. 14.0 (SPSS Inc., Chicago, IL, USA) for Windows was used for the statistical analysis, and p-values less than 0.05 were considered statistically significant.
RESULTS
1. Relationship between the expression of B7-H4 and clinical and pathological characteristics
The mean age of the study group was 53.0±12.0 years (range, 31-74 years). The mean postsurgical follow-up period was an average of 33.4±21.0 months (range, 6-84 months). Males and females accounted for 39 patients (38.2%) and 63 patients (61.8 %), respectively. The immunohistochemical staining showed that the group with expression of B7-H4 and the group without expression included 18 (17.6%) and 84 patients (82.4%), respectively. In the group with expression of B7-H4, 8 patients had a partial nephrectomy, and in the group without B7-H4 expression, 57 patients had a partial nephrectomy. Only 1 patient who had a partial nephrectomy had positive surgical margins; however, this patient did not have disease recurrence.
There was no significant difference between the groups with and without B7-H4 expression with regard to age, gender, symptoms at the time of diagnosis, tumor size at the time of diagnosis, TNM disease stage, lymphovascular invasion, or nuclear grade (Table 1).
2. Relationship between the expression of B7-H4 and recurrence rate
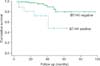
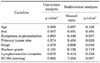
Among the 102 patients, in 5 out of 18 patients (27.8%) who were positive for the expression of B7-H4, lymph node metastasis and distant metastasis developed during the follow-up period. Among 84 patients negative for the expression of B7-H4, 7 patients (8.3%) developed disease recurrence; there was a higher recurrence rate in the B7-H4-positive group (p=0.035). Among the factors studied for their association with disease recurrence, only the expression of B7-H4 showed a statistically significant relationship by univariate analysis (Fig. 2). The multivariate survival analysis for postsurgical disease recurrence showed that expression of B7-H4, tumor size, and disease stage were associated with disease recurrence (Table 2).
DISCUSSION
Several types of genes, proteins, and growth factors have been associated with the prognosis of patients who have RCC [4]. One such factor, carbonic anhydrase IX (CAIX), is a prognostic factor that has been widely investigated. By controlling intra- as well as extracellular acidity, CAIX plays an important role in the adaptation of cells to hypoxic environments. According to Bui et al, CAIX was shown to be an independent prognostic factor for the tumor-specific survival rate, and regardless of the disease stage of the tumors or their histological grade, the probability of death in cases with a low expression of CAIX was approximately three times that than in cases with a high expression [12]. However, in another study performed on 730 patients with clear cell RCC, the multivariate analysis did not confirm that CAIX was an independent prognostic factor [13].
Aberrant expression of the insulin-like growth factor mRNA binding protein (IMP) family member IMP-3 has been demonstrated in several human malignancies [14]. The role of IMP-3 in tumorigenesis is thought to involve the promotion of cellular proliferation. IMP-3 expression was a significant independent predictor of metastasis-free and overall survival after multivariate adjustment. These findings were validated by Hoffmann et al in a study of 716 consecutive patients with clear cell RCC examined for IMP-3 expression; 88% (629 of 716) of the specimens examined had pathologically localized disease at the time of nephrectomy [15]. Among the pathologically localized tumors, 26% (163 of 629) stained positive for IMP-3. The 5- and 10-year progression-free survival rates were significantly lower in patients with IMP-3-positive tumors than in patients with IMP-3-negative tumors (51% and 41% vs. 89% and 82%, respectively).
Survivin is an antiapoptotic protein that is overexpressed in almost all human malignancies; it is rarely detected in normal tissue. Survivin is believed to inhibit both the intrinsic and extrinsic caspase cascades. Survivin expression has been correlated with several adverse pathological features of clear cell RCC, including tumor size, nuclear grade, TNM classification, presence of metastatic disease, coagulative tumor necrosis, and sarcomatoid differentiation [16]. Moreover, in a series reported by Parker et al, 312 patients with high survivin expression were twice as likely to die from clear cell RCC as were patients with low survivin expression [16].
The B7 family plays an important role in the regulation of antigen-specific T cell-mediated immune reactions. The expression of such proteins is limited to phagocytic and lymphoid cells [17]. The expression of B7-H4 and B7-H1 in several tumors, including clear cell RCC, has been reported; they have been associated with blocking effective anti-tumor immune mechanisms and with an increased risk of tumor-specific death [18]. Several studies have demonstrated the expression of B7-H4 in clear cell tumors of the kidneys [19]; these findings were confirmed in this study. The results of this study showed that tumor recurrence was more common in patients with B7-H4 expression.
B7-H4 has been shown to be a suppressor of the T cell-mediated immune response [6-8]. Several studies have reported that B7-H4 acts directly on apoptotic mechanisms associated with tumor cells. In particular, in ovarian tumors, B7-H4 has been reported to accelerate tumor formation. In breast tumors, the expression of B7-H4 mRNA and protein were blocked in vitro, and this was associated with the acceleration of apoptosis of tumor cells [20]. Therefore, B7-H4 appears to act by two different mechanisms. One is as a negative regulator of cell-mediated antitumor activity, and the other is by the unresponsiveness of tumor cells to apoptosis. B7-H4 suppresses the proliferation of CD4 and CD8 T cells as well as the secretion of cellular hormones. The receptors are thought to be the B and T lymphocyte attenuator (BTLA) expressed on activated T cells [21]. These mechanisms enhance disease progression and tumor activity. However, studies on the mechanism of B7-H4 activity are in early stages, and further research is needed.
The results of this study confirmed the expression of B7-H4 in clear cell RCC. Previous studies reported the sporadic expression of B7-H4 in the distal convoluted tubules [22]. However, the expression of B7-H4 in the proximal convoluted tubules has not been reported [23,24]. In addition, the expression of B7-H4 has been associated with lymphocyte infiltration and a poor prognosis in patients with cancer [25]. Moreover, in this study, the expression of B7-H4 was shown to increase the risk of recurrence in patients with localized RCC.
Currently, the role of genetic factors and molecular markers has been limited in the diagnosis and management of patients with renal cell cancer. However, in the future, advancements in imaging technology as well as immunotherapy in combination with genetic studies might improve the treatment and management of patients with renal cell cancer, such as with sunitinib and sorafenib [26].
Molecular biomarkers can assist with the diagnosis of a malignancy, may represent potential therapeutic targets, and may offer a means to monitor disease recurrence after treatment. Moreover, selected biomarkers may prove useful when incorporated into existing risk stratification models to help clinicians more accurately counsel patients regarding disease prognosis. Clinically, the use of molecular markers has several problems. The molecular markers require immunohistochemical staining of tumor tissues. Biological markers that could be used on serum and urine samples would be more accessible for the assessment of response to therapy as well as for tumor surveillance [27].
The limitations of this study include the following. This study was a retrospective chart review. According to previous reports [5], the expression of B7-H4 was 59.0%, and in this study it was 17.6%. This low expression rate is thought to be due to the immunohistochemical staining method used to assess the expression of B7-H4 in paraffin-embedded tissues. Many previous studies used fresh frozen samples. In addition, the study subjects in this report represented clinical disease limited to stage T1. Furthermore, the sample size was relatively small.
CONCLUSIONS
The results of this study showed that the expression of B7-H4 was associated with the prognosis of patients with clear cell RCC and recurrence in patients with stage T1 tumors. Although multiple current prognostic models based on clinical and pathological variables exist, further improvements in the accuracy of such models may be achieved with the development and implementation of molecular biomarkers. The expression of B7-H4 might be used to manage patients with RCC and as a target for novel treatments.


 XML Download
XML Download