

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Ureter stone disease is one of the most common conditions seen in the emergency department, and the lifetime prevalence is estimated at 10% to 15% [1,2]. Patients with ureter stone disease usually complain of severe renal colic caused by sudden obstruction of the ureter by the stone. Ureter stone disease can be managed by conservative treatment, extracorporeal shockwave lithotripsy (ESWL), ureteroscopic removal of stone (URS), percutaneous nephrolithotripsy (PCNL), and laparoscopic or open surgery [3]. Although there are many factors to consider in the decision on the management of ureter stones, most patients are recommended to wait until spontaneous passage of a stone. However, during conservative management, patients may experience undesirable complications such as recurrence of renal colic and urinary infection. Several studies have shown that almost 40% of patients with ureter stone disease have difficulty passing their stone and often require an intervention [4,5].
Understanding the natural history of ureter stone disease is highly important for managing the patients, especially which patients will be able to wait until the stone is expelled and how long a patient should be observed to minimize undesirable complications. In this aspect, information on the location, size, and shape of the stone is essential in the selection of a proper treatment modality. Morse and Resnick reported that 60% of ureter stones passed spontaneously, and stones in the distal third of the ureter had a spontaneous passage rate of 45%, compared with the mid third of 22%, and the proximal third of 12% [6]. In another study, two thirds of all stones that passed did so within 4 weeks after the onset of symptoms [7]. However, these studies included a relatively small number of subjects or multicenter populations; thus, the value of direct comparative data was limited.
Although guidelines for the management of ureter stones were published by the American Urological Association [8], there have been no prior studies for predicting the spontaneous passage of ureter stones in Korean patients. The aim of this study was to evaluate the natural history of ureter stones and the clinical factors associated with stone passage in a long-term, single institution experience.
MATERIALS AND METHODS
We reviewed the charts of all patients who visited the emergency room or urological office of our institution with acute renal colic between 2001 and 2008. A total of 656 ureter stone formers in whom stones could be detected by intravenous urography (IVU) or computed tomography (CT) at initial the diagnosis and who had decided to be treated by expectant management on their own account or by our suggestion were enrolled in this study. Additionally, the patients underwent a series of measurements, including case history, physical examination, complete blood cell count, routine urinalysis, and serum creatinine measurement. Cases were excluded if the patients needed prompt management due to uncontrolled colicky pain or wanted early treatment or if consistent follow-up could not be made. In addition, patients aged less than 18 years, with urinary tract abnormality, with an impacted stone, with a radiolucent or not easily visualized stone on plain film, with urinary tract infection, with renal insufficiency, or taking α-blockers were excluded from this study.
The size of the ureter stone was defined as its longest diameter on KUB or CT scan. The location of the stones was classified as the upper ureter (between the renal pelvis and the upper border of the sacrum), the mid ureter (between the upper and lower border of the sacrum), and the lower ureter (between the lower border of the sacrum and the ureterovesical junction).
The follow-up was carried out every week to check for stone passage according to the patient's statement or radiologic examination with plain film and ultrasonography. The date of stone passage was defined as an identification or sense of stone passage by the patients themselves. In the case of patients who were unsure of the stone passing, patients who were symptom-free and with disappearance of the stone on radiologic study were considered as having spontaneous stone passage. The expectant management was continued until the patients complained of symptoms or there was evidence of progressive renal deterioration on radiologic study, even in the case of patients who were symptom-free.
We categorized the patients into 2 groups according to end results: group 1 experienced spontaneous passages of stones and group 2 underwent interventions. Clinical parameters such as gender, age, size and location of the stone, body mass index (BMI), and previous stone history were analyzed for stone passage time and differences between the groups. Continuous variables were assessed by using Student's t-test or one-way ANOVA test. Categorical variables were compared with the chi-square test or linear by linear association test. Log rank tests were used to analyze the association of spontaneous passage time and size and location of the stone. Statistical analysis was performed by using SPSS ver. 12.0 (SPSS Inc., Chicago, IL, USA), and p-values of <0.05 were considered statistically significant.
RESULTS
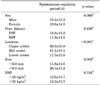
The baseline characteristics of the studied population are summarized in Table 1. The mean age of the patients was 42.6 years (range, 18 to 76 years) and the male to female ratio was 2.11 : 1. Of the 656 patients, 428 (65.2%) were first-time stone formers, and 576 (87.8%) had stones located in the lower ureter. Most of them had stones less than 6 mm in size. The mean size of the ureter stones was 3.9±1.8 mm (range, 1.7 to 20.0 mm) and about 95% of the ureter stones were less than 6 mm (data not shown). We assessed the time to stone passage from initial diagnosis to spontaneous stone passage according to clinical factors (Table 2). Duration for spontaneous passage showed a decreasing trend according to stone location (p<0.001). Small-sized stones had a significantly shorter time for spontaneous passage than did large-sized stones (p=0.002). The mean period of spontaneous passage for stones less than 2 mm in size was 6.8 days; that for stones 2 to 4 mm, 12.6 days; for 4 to 6 mm, 14.8 days; and for stones 6 to 8 mm, 21.8 days (p<0.001, data not shown). The cumulative spontaneous passage rate was 55.3% in 7 days, 73.7% in 14 days, 91.5% in 30 days, and 97.7% in 56 days after the first attack (Fig. 1). Fig. 2A shows the spontaneous stone passage rate between small-sized stones and large-sized stones during the observational periods. Stones 6 mm or larger had only a 57.5% chance of spontaneous passage within 2 months of the expectancy period, and stones smaller than 6 mm had an 88.7% chance of spontaneous passage in the same period. The passage rates were similar at 2 and 3 months for both smaller and larger stones. During follow-up, lower ureter stones had a higher spontaneous passage rate than did upper and mid ureter stones. In the case of lower ureter stones, the chances of spontaneous passage were similar at 2 and 3 months (Fig. 2B). Considering both size and location of stones, the patients with proximal site and large-sized stones (≥6 mm) had a lower chance of passing the stones spontaneously than did the other groups (log rank test, p<0.001) (Fig. 2C).
A total of 90 patients needed intervention because of a colic attack in 30 patients (ESWL in 18, URS in 11, and ureterolithotomy in 2) and persistent or progressive renal deterioration in 60 patients (ESWL in 40 and URS in 20). In the comparison between the spontaneous passage and intervention groups, no significant differences were found in age, sex distribution, BMI, or previous stone history (p>0.05). The patients in the intervention group had a significantly larger stone size than did those in the spontaneous passage group (3.6±1.5 vs. 5.5±2.7 mm, p<0.001). Compared with the intervention group, patients having spontaneous stone passage had a higher prevalence of lower ureter stones (p<0.001). The frequency of small-sized stones (<6.0 mm) was also higher in the spontaneous passage group (Table 1).
DISCUSSION
We investigated the outcome of ureter stones in patients treated by expectant management and found that the stone's size and location are the most important clinical factors for predicting the spontaneous passage of ureter stones during expectant management. Time to spontaneous passage increased according to the size of the stone, and stones larger than 6.0 mm needed more than 20 days for spontaneous passage.
Although various techniques for ureter stone management are available, expectancy until the stone expels is the most common management option in ureter stone disease. However, it is very difficult to decide how long patients should wait for stone passage and when physicians should start more invasive intervention. For this reason, there have been many efforts to identify the natural history of ureter stones. In 1977, Ueno et al evaluated 520 patients and calculated the rate of spontaneous passage of ureter stones as a function of stone width and length (in 1 mm increments) [9]. They found that the degree of obstruction was more directly related to the width rather than the length of the stone and concluded that the width was the critical measurement. Passage rates were 100%, 93%, 87%, and 78% for stones measuring 1, 2, 3, and 4 mm in width, respectively, and the rate dropped to 57% for stones 5 mm in width, 35% for 6 mm stones, 28% for 7 mm stones, and 14% for 8 mm stones. No stones exceeding 8 mm in width passed spontaneously. In the current study, the size of the ureter stone was defined as its longest diameter on KUB or CT scan. Stones 6 mm or larger had only a 57.5% chance of spontaneous passage within 2 months of the expectancy period. On the other hand, stones smaller than 6 mm had an 88.7% chance of spontaneous passage in the same period. Although most urologists usually recommend delaying definite treatment by 4 weeks for patients with ureter stones on expectant management, our results showed that the passage rates were similar at 2 months and 3 months during the follow-up period. This finding suggests that the expectancy period may be sustained until 2 months in selected patients.
Likewise, the locations of stones also have been well recognized as an important factor in the spontaneous expulsion rate. In 1991, Morse and Resnick determined the frequency of spontaneous passage for ureter stones in a series of 378 patients and reported an overall frequency of spontaneous passage of 60% [6]. The frequency was related to stone location: 22% for upper ureter stones, 46% for mid ureter stones, and 71% for lower ureter stones. Miller and Kane suggested that interval to stone passage is highly variable and dependent on stone size, location, and side [10]. In our study, lower ureter stones showed an 88.1% passage rate in 4 weeks and a similar rate until 3 months of observation. In case of upper and mid ureter stones, the passage rate was increased until 2 months and was similar at 3 months. These results suggest that intervention may be held until 4 weeks for distal stones and until 2 months for proximal stones.
The current study revealed that the size and location of ureter stones are the most important factors and have a nearly linear relationship with the frequency of spontaneous passage. These results are very similar to those of prior studies reported in the literature. In the Korean population, however, no guidelines for selecting the optimal therapeutic approach for ureter stones have been reported. Few studies have concerned the efficacy of expectancy for ureter stones. In 1992, Choo et al reported that of 78 calculi treated with expectation, 58 (74.4%) passed spontaneously [11]. They concluded that it is preferable to treat upper ureter stones smaller than 6 mm and lower ureter stones smaller than 7 mm with expectation until 3 months and 5 weeks, respectively. In 1995, Min and Shin reported the treatment option for lower ureter stones [12]. In their study, 37 were treated by expectancy only. They recommended initial expectancy for up to 3 weeks for lower ureter stones smaller than 10 mm. In contrast with our current study, these reports enrolled only a small study population and the results were derived from periods when noninvasive therapeutic modalities (URS or ESWL) were not popularized, just initiated.
In this study, a total of 90 patients (13.7%) required interventions because of symptom relapse or renal deterioration that was also related to the location and size of the stones. The more proximal the location of the stone and the larger the stone was than 6 mm, the less the chance of spontaneous passage. It is very important to determine optional and objective criteria for choosing an appropriate treatment modality for ureter stones. Nowadays, new technology has been introduced [13-17], and some investigators have tried to adapt the medical expulsive therapy for ureter stones [18-20]. Although these developments may relieve the pain or enhance the quality of life among patients with urolithiasis, the burden of the cost is not cheap. Therefore, our large-scale, long-term observational study has a crucial role for selecting a treatment modality for ureter stones.
This study had several kinds of inevitable limitations. Our results revealed that spontaneous passing of the stone occurred in 86.3% and the mean time to stone passage was 12.5 days. This may not reflect the true interval and rate of stone passage and the real time is expected to be shorter than we investigated because the date of stone passage was recorded as the visit date for patients who were unsure of stone passage. However, we think that the observational error will be narrow because of our frequent follow-up schedule. Also, we believe that this study is valuable because no studies have previously been performed in a large-scale, long-term observational manner in Korea. From our study, we have suggested appropriate guidelines for managing patients with ureter stones in the Korean population and our study will be a cornerstone cited by other new studies.
CONCLUSIONS
Stone size and location are the most important factors for predicting the likelihood of spontaneous passage of ureter stones in patients on expectant management. If a patient has a distal ureter stone of less than 6 mm, it is acceptable for the urologist to observe for spontaneous passage for 2 months. We suggest that proximal ureter stones of more than 6 mm in size require early treatment within 1 month.



 XML Download
XML Download