

 PDF
PDF ePub
ePub Citation
Citation Print
Print


The advantages of laparoscopic surgery over open surgery include a better cosmetic outcome, less postoperative pain, and a shorter hospital stay. However, laparoscopic surgery is more difficult to perform than is conventional open surgery. Developed as an extension of conventional laparoscopy, most operations within the field of urology can be performed with the use of laparoscopic techniques. Recently, a new procedure was developed-laparoendoscopic single-site surgery (LESS) with a single incision around the umbilicus-that has the potential to replace conventional laparoscopic surgery. Kaouk et al have already reported that LESS may result in a more rapid return of patients to normal activity [1]. Herein, we report the use of concomitant LESS for ureterolithotomy and contralateral renal cyst marsupialization for the treatment of a patient with a right ureter stone and a left renal cyst.
CASE REPORT
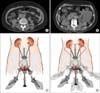
A 63-year-old woman presented to the emergency room with severe right-flank pain that had developed 12 hours earlier and left-flank pain with dull and intermittent characteristics. She had received medication at another hospital for tuberculosis pleurisy 20 years previously and had undergone vertebroplasty for compression fracture of the lumbar vertebra 3 years previously. On physical examination, right costovertebral angle tenderness was noted. Urinalysis indicated microscopic hematuria, and the results of an initial blood test and chest X-ray were normal. Radiographs of the kidney, ureter, and bladder showed an irregular-shaped calcification of approximately 1.5 cm along the ureter course around the upper portion of the third lumbar verterbra. Computed tomography (CT) identified a right ureter stone measuring 1.3x0.6 cm and hydronephrosis of the right kidney. CT also identified a 7 cm simple cyst located at the anterior aspect of the left midpole kidney, which was classified as Bosniak category I (Fig. 1A, B). To decompress the hydronephrosis, we attempted to insert a double-J stent; however, we could not insert a road-runner guidewire because the guidewire was bent at the level of the stone under fluoroscopy. This problem raised suspicion of the existence of an impacted stone. Preoperatively, we explained the various procedures and techniques available to the patient, including the use of a homemade single-port device. The patient provided signed informed consent to undergo concomitant LESS ureterolithotomy and contralateral marsupialization.
SURGICAL TECHNIQUE
Under general anesthesia, the patient was placed in the flank position with the left side elevated by 70°. A 3 cm crescenteric marginal skin incision around the umbilicus and a 1 cm extended fascial incision were made. We used a small Alexis® wound retractor (Applied Medical, Rancho, Santa Margarita, CA, USA) and a powder-free surgical glove (Triplex P-free Glove®; KM Healthcare, Guri, Korea) to insert the homemade single-port device (Fig. 2A). The wound retractor was inserted at the site of the single incision. The homemade single-port device was constructed by fixing and rolling the surgical glove to the outer ring of the wound retractor so that it would not fall off; two 12 mm trocars and a 5 mm trocar were used to secure the fingers of the size 6 1/2 surgical glove to the end of three trocars with a silk 1-0 suture. A 10 mm rigid laparoscope (30°) was inserted through the middle 12 mm trocar, and the laparoscopic instruments were inserted through the other two trocars because the 5 mm and 10 mm flexible laparoscopes were not equipped for insertion. Two flexible laparoscopic instruments (LaparoAngle®; CambridgeEndo, Framingham, MA, USA) were inserted and configured in revere alignment ("mirror-imaging"); conventional rigid instruments were used occasionally. After dissection of Gerota's fascia, renal cyst fluid was aspirated by tapping. The cystic fluid underwent cytologic and chemical testing, and its color and volume were assessed (Fig. 2B). The cystic wall was resected and sent out for histologic analysis. The remaining renal cystic wall was electrocauterized to prevent recurrence. After the LESS technique on the left side of the patient was completed, the patient was repositioned to expose the right side (Fig. 1C, D). The repositioning to the right side took approximately 20 minutes. After resection of the line of Toldt, the large intestine was tacked to the medial side and the ureter was exposed within the peritoneum. After the location of the stone was determined, a longitudinal incision was made with a pair of laparoscopic Metzenbaum scissors. The ureter stone was extracted easily and rapidly with laparoscopic forceps through one finger of the device. The vertically resected ureter was closed with an uninterrupted 5-0 polyglactin suture, and a drainage tube was placed at the anastomosis site of the ureter (Fig. 2C). A double-J stent was inserted with cystocopy and fluoroscopy after skin suture. The surgical procedure lasted 210 minutes (left side: 50 minutes; right side: 160 minutes), and the estimated blood loss was 100 ml. Postoperatively, the patient was able to tolerate a diet and received no self-administered analgesia. On postoperative day 4, the drainage tube was removed, and the patient was discharged home. No complications were observed during the postoperative period. On postoperative day 21, the ureteral stent was removed. A diagnosis of simple renal cyst was made on the basis of pathologic and cytologic examination. The patient experienced no complications after removal of the ureteral stent and did not complain of right- or left-flank pain.
DISCUSSION
The LESS technique was first attempted and reported on approximately 10 years ago. However, the rate of surgical success at that time was very low, which inhibited the widespread use of LESS. Recently, conventional laparoscopic surgery has undergone changes with the goal of achieving a minimally invasive surgical technique. This goal has recently born fruit with the development of new techniques such as natural orifice transluminal endoscopic surgery (NOTES™) and LESS. Since the founding of the Laparoendoscopic Single-Site Surgery Consortium for Assessment and Research (LESSCAR) in 2008, laparoscopic surgery through a single incision site has been termed "LESS" [2]. Conventional laparoscopic surgery requires 3 to 4 transcutaneous ports and an additional opening in some cases to extract a resected organ. Because of the use of port devices only in the umbilicus, this laparoscopic procedure is more difficult to perform than are conventional laparoscopic procedures and other older techniques. However, LESS is associated with minimal pain and with a barely visible wound because of its use of only a single incision around the umbilicus [3].
In bilateral surgery, a single incision is one of the most important advantages because the procedure can be performed without the placement of an additional port after repositioning the patient. Recently, Jeong et al described a case of bilateral LESS adrenalectomy for an aldosterone-producing adrenal adenoma [4]. They used an OCTO Port (Dalim SurgNet, Seoul, Korea) and a 5 mm flexible-tip laparoscope. They concluded that LESS is the optimal technique for bilateral surgery. One of the key advantages of bilateral LESS is that only one incision site is needed. In addition, homemade single-port devices can be used for bilateral surgery with LESS. Compared with commercialized single-port devices, homemade single-port devices composed of a wound retractor and a surgical glove have the advantage of allowing the laparoscope and instruments to move freely in a limited space during bilateral surgery. Furthermore, the elasticity of the surgical glove minimizes the possible interference of instruments with the laparoscope during bilateral surgery. If additional surgical instruments are needed, another finger of the glove can be cut for their insertion. When a lesion is located in the upper pole of the kidney, and thus is covered by the liver or spleen, traction can be performed with the use of rigid instruments through an additional trocar. Some disadvantages of the LESS technique include the time needed to construct the device, the possible entrapment of instruments in the abdominal wall when inserted through the trocar, and the failure of sutures to achieve good triangulation [5]. Great care should be taken to prevent contamination of the port device when the patient is repositioned during bilateral surgery.
No complications developed during or after concomitant left renal cyst marsupialization and right ureterolithotomy with the LESS technique and the use of a homemade single-port device. The patients were very satisfied with their outcomes, because they experienced minimal pain and their wounds were barely visible.
LESS is a new technique that is not yet widely used. However, because the complications associated with LESS are no greater than those associated with conventional laparoscopic surgery, we expect higher levels of patient satisfaction with LESS. Arguably, LESS is more efficient than conventional laparoscopic surgery at treating bilateral diseases because additional ports are not needed.

 XML Download
XML Download