

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Cystic dysplasia of the testis (CDT) is an uncommon cause of testicular masses that is often associated with renal and other genitourinary tract anomalies during childhood [1,2]. It was first described by Leissring and Oppenheimer [2] in 1973, and since then approximately 50 additional cases have been reported [3]. CDT consists of multiple irregular, small cystic spaces, originating in the mediastinal area, and affects either a part of or the whole testis [1,4,5]. This results in enlargement of the testis and atrophy of the remaining parenchyma. We experienced a CDT in a 63-year-old man with a direct inguinal hernia. To our knowledge, this is the first report in the published literature documenting incidental CDT in an aged patient.
CASE REPORT
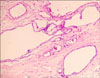
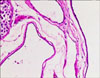
A 63-year-old man with left inguinal bulging during increased abdominal pressure visited our urologic department. He did not complain of scrotal swelling or discomfort, and he had no significant medical history. In the physical examination, a soft mass was palpated in the left inguinal area during the Valsalva maneuver, but there were no abnormal findings on the scrotum. Ultrasonography showed a left direct inguinal hernia in the inguinal area and a well-circumscribed cystic lesion containing multiple minute cysts with echogenic foci occupying almost one-third of the left testicular parenchyma (Fig. 1). The testes were symmetrical in size on ultrasonography. Considering the age of the patient, the cystic lesion in the left testis was presumed to be a malignant testicular tumor rather than a benign tumor. Testicular tumor markers (α-fetoprotein, human chorionic gonadotropin, and lactate dehydrogenase) were within normal limits and a computed tomography scan of the abdomen showed no remarkable findings. Left radical orchiectomy with herniorrhaphy was performed. By gross examination, the left testis measured 3.7×3.3×2.8 cm. A localized, ill-defined, multilocular, noncommunicating, microcystic lesion exclusively involving the testicular parenchyma at the mediastinum testis was confirmed. Microscopic examination showed irregular cystic spaces lined by flattened cuboidal nonciliated epithelium with no nuclear atypia and relatively well-preserved seminiferous tubules with the absence of any tubular atrophy, basement membrane thickening, interstitial fibrosis, or Leydig cell hyperplasia. There were no specific findings in the epididymis, vas deferens, or paratesticular soft tissue (Fig. 2, 3). The pathologic diagnosis was a CDT on the left testis.
DISCUSSION
CDT is a rare benign testicular tumor that presents predominantly in childhood [1,2]. The mean age of presentation is 6.1 years (range, 0-23 years) [1]. However, the patient in the present case was 63 years old. To our knowledge, based on a review of the literature, this is the first case in which CDT was found in an old age group.
CDT is thought to be a congenital lesion that is often associated with genitourinary anomalies, of which ipsilateral renal agenesis (51%) is the most common. Only 3 cases (6%) have been confirmed to have no associated anomalies [1,4-6]. Therefore, upper urinary tract evaluation is needed to confirm the associated genitourinary anomalies. The cause of genitourinary anomalies is estimated to be a mesonephric duct development disorder resulting from a lack of connection between the efferent ductules and the rete testis, leading to degeneration of the mediastinum testis into cysts with progressive ductal dilatation and compression or replacement of adjacent testicular tissue [1,3-5]. Therefore, the most common symptom presented by the patient with CDT is scrotal swelling. In the present case, however, the patient's chief complaint was left inguinal bulging, and the cystic lesion of the testis was found incidentally during a work-up for an inguinal hernia.
Typical sonographic findings of CDT are multiple small cysts in the range of 2-8 mm, with a compressed contour of normal testicular tissue [1,5,7,8]. However, an accurate diagnosis of CDT by ultrasound in adults is difficult because CDT, cystic ectasia, and malignant tumors appear similarly on ultrasonography [1]. In the pathologic examination of CDT, irregular cystic spaces are lined by flattened cuboidal nonciliated epithelium and septations by connective tissue [3-5], which coincides with the pathologic findings in the present case.
Cystic lesions of the testis in children are usually thought to be nonobstructive congenital anomalies, whereas 75% of cysts in adults are thought to be of an obsturctive etiology, for example, efferent duct or epididymal obstruction due to an inguinal hernia [1,9]. Cystic ectasis is an acquired disease that can be associated with and occur as a result of mechanical compression of the epididymis or spermatic cord by surgical, traumatic, neoplastic, or infectious processes and ischemic or hormonally induced atrophic alterations in epididymal tubules [8]. In the present case, however, there was no evidence of etiologies of cystic ectasis in the pathological examination as mentioned above. With respect to the diagnosis of CDT, Kogan has suggested diagnostic criteria that include a typical cystic lesion on ultrasonography, normal testicular tumor markers, and associated urogenital anomalies [8]. If these criteria are met, he recommended that open excision is unnecessary for diagnosis. However, the present case did not meet these criteria and the patient was an aged man with an accompanying inguinal hernia; therefore, surgical excision was considered.
The gold standard treatment of CDT has yet to be established. Treatment options are radical orchiectomy, testicular-sparing cyst excision, and active surveillance [1,3,8,10]. Radical orchiectomy has been the treatment of choice because it is difficult to differentiate CDT from other cystic testicular tumors [1,3,8,10]. Also, in the present case, the sonographic findings of the left testis were similar to the typical findings of CDT as mentioned above, but considering the age of patient and the lack of evidence of associated urogenital anomalies, the differential diagnosis of CDT from other malignant tumors was difficult. Therefore, left radical orchiectomy was performed. However, if the diagnostic criteria of CDT are met, more conservative approaches should be advocated with further understanding of the disease characteristic of CDT and consideration of its benign nature.
To our knowledge, this is the first report in the published literature documenting the incidence of CDT in old age. Therefore, we report this case as a reminder that CDT can occur in old age groups and should be considered as a diagnosis before performing radical orchiectomy.

 XML Download
XML Download