

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Although about 80% of patients with non-muscle-invasive bladder cancer can be successfully treated through surgery and adjuvant intravesical therapy, two-thirds of patients experience tumor recurrence within 5 years, and high-grade T1 tumors and carcinoma in situ have the potential to progress and possibly metastasize [1]. Patients with in vasive bladder cancer require a radical cystectomy. However, it is controversial whether neoadjuvant or adjuvant chemotherapy improves survival in patients with invasive bladder cancer, even though bladder transitional cell carcinoma is relatively chemotherapy-sensitive. Thus, during the past few decades, numerous trials have been conducted to develop new treatment regimens for both superficial and invasive bladder cancer, because there is an urgent need to identify new agents to prevent bladder cancer recurrence and progression [2-5].
The mammalian target of rapamycin (mTOR), a ubiquitous serine-threonine kinase and a downstream component of the phosphatidylinositol 3'-kinase (PI3K)/AKT/phosphatase and the tensin homologue (PTEN)-signaling pathway, has been shown to play a critical role in the regulation of protein synthesis, cell growth, proliferation, apoptosis, survival, and angiogenesis [6]. Furthermore, mTOR has also been demonstrated to act as a transitional activator of hypoxia-inducible factor (HIF) through its activated downstream molecules, namely phosphorylated S6 protein (phosS6) and phosphorylated eukaryotic translation initiation factor 4E-binding protein-1 (phos4E-BP1) [7]. Indeed, elevated mTOR pathway activity has been noted to be important in a variety of human tumors both in vivo and in vitro and in bladder cancer in vitro [8-12].
In this study, we investigated the expression and reciprocal interplay of three mTOR pathway-related markers (mTOR, phosS6, and phos4E-BP1) to determine the prognostic and biological significance of these mTOR pathway-related markers in patients with bladder cancer who had undergone transurethral resectioning of their bladder tumor (TURB) as well as radical cystectomy.
MATERIALS AND METHODS
1. Patient cohort and tissue microarray construction
After obtaining institutional review board approval, we retrieved 208 bladder cancer specimens collected at Chung-Ang University Hospital between 1989 and 2007. We excluded samples from patients who had a history of preoperative treatment including radiotherapy, systemic chemotherapy, or intravesical therapy. All sections were reviewed to confirm the original diagnosis and were then staged according to the 2004 American Joint Committee on Cancer (AJCC)/Union International Contre le Cancer TNM, 6th Edition Pathology Reporting Protocol, including TNM and AJCC stages. Grading was performed at the time of surgery by using either the World Health Organization/International Society of Urological Pathology consensus classification or the 1965 classification [13,14]. Given the different grading systems used during the span of our study, standardization was performed by an expert urologic pathologist (TJ Lee), who classified all tumors as either high-grade or low-grade for statistical analyses. Paraffin blocks were available for 208 cases, and tissue microarrays (TMAs) were constructed by using a manual array device (TMA set, Labro, Seoul, Republic of Korea). Two-millimeter-thick triplicate tumor samples were spotted from each sample, and 35 triplicate benign urothelium samples were obtained from the benign regions. Four-micrometer-thick sections were consecutively incised from the recipient block and transferred to polylysine-coated glass slides. Hematoxylin and eosin staining was performed on the TMAs to confirm the presence of tumor tissue or benign urothelium.
2. Clinicopathological data
All patients' clinicopathological data were retrieved from electronic medical records. These included patient demographics and preoperative information such as diagnostic procedures and clinical stage. Follow-up data on disease recurrence, progression, disease-specific survival (DSS), and overall survival (OS) were obtained by review of patient medical records, letters of inquiry to patients, and a review of the social security death index. For patients who had undergone partial or radical cystectomy, pelvic recurrence as well as recurrent metastatic disease were considered to be progression events.
3. Immunohistochemistry
For the immunohistochemical procedures, 4 µm-thick sections were deparaffinized, rehydrated, and subjected to heat-induced antigen retrieval with buffer solution using a streamer autoclave. Sections were then incubated with the appropriate primary antibody. After the application of a secondary antibody, slides were developed using the chromogen 3-3'-diaminobenzidine and counterstained with hematoxylin. Table 1 lists all pertinent marker information, including vendor, clone, dilution, pretreatment and incubation conditions, staining site, and positive controls. TMA spots with artificial folds or those lacking target tissue representation were omitted from further analyses. Tumors and benign TMA spots stained with each marker were evaluated for patterns of staining (nuclear vs. cytoplasmic), extent (percent of positive cells), and intensity (0 to 3+ score). An H-score was generated for each marker as the sum of the products of each intensity category multiplied by the extent of immunoexpression [15]. A final H-score was generated by taking the average of triplicate tissue samples. The H-scores of markers were used in the statistical analyses. In univariate and multivariate analyses, a cutoff value of expression of each marker was used according to the mean tumor H-score (H-score≥141, 125, and 44, for mTOR, phos4E-BP1, and phosS6, respectively). We defined strong expression of a marker as expression equal to or greater than the cutoff value, and weak expression as no expression or expression less than the cutoff value.
4. Statistical analysis
SPSS ver. 14.0 (SPSS Inc., Chicago, IL, USA) was used for all statistical analyses. Differences between two variables were investigated by using a two-tailed Student's t-test, and ANOVA analysis was used when comparing more than three variables. Pearson correlation coefficients were calculated to test relationships among parameters. Recurrence-free and progression-free survival curves were estimated by using the Kaplan-Meier method, and any differences in the survival curves were compared by log-rank tests. A Cox regression model was used during multivariate analysis and p<0.05 was considered significant.
RESULTS
1. Demographic, clinical, and treatment characteristics
The median age at diagnosis for the patient cohort was 67 years (range: 29-87 years) with a male to female ratio of 9:1 and a median follow-up period of 72 months (range: 1-257 months). In our cohort, 154 patients (74%) were diagnosed with carcinoma in situ or superficial bladder cancer and 54 (26%) with invasive or metastatic bladder cancer. One hundred sixty patients (76.9%) had undergone TURB, and 46 (22.1%) had undergone partial or radical cystectomy. Recurrence was observed in 88 patients (42.3%) and progression in 53 (25.5%). Rates of OS and DSS were 54.8% and 78.4%, respectively.
2. Expression of mTOR pathway-related markers in relation to clinicopathological variables
As shown in Fig. 1A, mTOR, phos4E-BP1, and phosS6 were expressed in the cytoplasm of bladder cancer cells and in benign urothelium. Overall, mTOR expression was detected in 197 (94.7%) of 208 bladder cancer samples and in 31 (88.6%) of 35 benign samples. Phos4E-BP1 and phosS6 were expressed in 96.2% and 72.6% of bladder cancer cohort samples, respectively, and in 71.4% and 94.3% of benign cohort samples, respectively. The mean H-score of phos4E-BP1 was higher in the bladder cancer cohort (125.5 vs. 61.2) than in the benign cohort, whereas the mean H-score of phosS6 was lower in the bladder cancer cohort than in the benign cohort (44.0 vs. 183.8). The H-score of mTOR was not significantly different between these two cohorts (141.0 vs. 141.9) (Fig. 1B). In the univariate analysis, there was no relationship between the H-scores of the markers and age, sex, or TMN stage grouping; however, the mean H-score of phosS6 expression was significantly higher in high-grade bladder cancer samples (63.0 vs. 27.0, p<0.01). Levels of the other two markers were not related to tumor grade (Table 2).
When we investigated the correlation between the expression of mTOR pathway-related markers, we found a significant positive correlation between mTOR and phos4E-BP1 H-scores (correlation coefficient, r=0.37, p<0.01), as well as between mTOR and phosS6 H-scores (r=0.17, p<0.05), although the correlation coefficient between mTOR and phosS6 was weak. Fig. 1C shows the mean H-scores of phosS6 and phos4EBP1 in relation to mTOR H-scores in bladder cancer. The mean H-scores of phos4EBP1 were significantly higher in cancer cells that strongly expressed mTOR than in cancer cells with no or weak mTOR expression (p<0.05). The mean H-scores of phosS6 were higher.
3. Univariate and multivariate survival analyses
Table 3 shows the results of the univariate and multivariate survival analyses. In the univariate analysis, a higher TNM stage and a higher cell grade were significant predictors of shorter progression, DSS, and OS. Furthermore, older age was associated with shorter progression and OS (p<0.05), although older age was of borderline significance in predicting DSS (p=0.080). Among mTOR pathway-related markers, only phosS6 was a significant predictor of progression, DSS, and OS, although mTOR was a predictor of OS, and phos4E-BP1 was a predictor of DSS. In the multivariate analysis, TNM stage and age remained independent predictors of progression, DSS, and OS, but not of tumor cell grade. Among the markers, strong phosS6 expression predicted shorter progression (p<0.01; hazard ratio [HR], 2.516) and DSS (p<0.01; HR, 2.396), but not OS (p=0.112), whereas strong phos4E-BP1 expression was a predictor of DSS (p<0.05; HR, 2.105).
4. Correlation between mTOR pathway-related marker expression status and progression-free survival and recurrence-free survival in patients with superficial bladder cancer
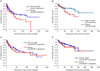
Of 154 superficial bladder cancer patients, 145 had undergone TURB, and in these patients, we investigated the correlation between mTOR pathway-related marker expression and progression-free survival and recurrencefree survival. The median age of this cohort was 64 years (range: 29-85 years) with a male to female ratio of 8.5:1.5 and a median follow-up of 72 months (range: 1-257 months). In our cohort, recurrence was observed in 59 patients (40.7%) and progression in 35 (24.1%). Kaplan-Meier survival analysis revealed that of the three mTOR-related markers, only strong phosS6 expression predicted shorter recurrence-free (p=0.046) and progression-free survival (p=0.035), although the p-value was not strong (Fig. 2).
DISCUSSION
It is well established that bladder cancer develops along two major molecular tracks [16]. The first track is characterized by the development of papillary lesions that rarely become invasive or metastatic but almost always recur [16]. These superficial tumors are therefore rarely lethal, but their high recurrence rates coupled with patient longevity have made them the most expensive solid tumors to treat and, therefore, a significant public health burden. Superficial tumors are thought to be driven by Ras pathway activation, most often (in up to 65% of cases) via the accumulation of activating mutations in the type 3 fibroblast growth factor receptor and less often via mutations in PI3K or Ras [17-19]. The second progression track involves the inactivation of major tumor suppressors [p53, Rb, and PTEN], which produces tumors that are highly invasive and metastatic [16,19]. Furthermore, PTEN loss leading to activation of the mTOR pathway has been reported in other genitourinary tract tumors such as prostate adenocarcinoma, renal cell carcinoma, upper tract urothelial carcinoma, and bladder urothelial carcinoma, offering a rationale for the limited but promising response of these types of tumors to mTOR inhibitors [20-24].
In our study, phos4E-BP1 expression was higher and phosS6 expression was lower in the bladder cancer cohort than in the benign cohort, although mTOR expression was not significantly different between these two cohorts. Schultz et al reported lower phosS6 expression in a bladder cancer cohort than in a benign urothelium cohort in a study of 144 bladder cancer patients who had undergone radical cystectomy [25]; they suggested that their findings were consistent with reduced activation of AKT, resulting in an overall down-regulation of the mTOR pathway. In our study, we observed a similar phosS6 expression pattern to that reported by Schultz and colleagues; however, in our study, the expression of mTOR was not increased. If these effects are due to down-regulation of mTOR, mTOR (nonactivated form) expression should have been elevated in bladder urothelial carcinoma samples compared with benign urothelium samples. Moreover, in our study, the bladder cancer cohort exhibited higher expression of phos4E-BP1 than seen in benign epithelium, indicating that the mTOR pathway was active. We believe that high phos4E-BP1 expression may be related to bladder cancer tumorigenesis. 4E-BP-1 is a protein that binds to the eukaryotic translation initiation factor4E (elF-4E) and plays a critical role in the regulation of gene expression. When 4E-BP1 is nonphosphorylated, it has been shown to bind tightly to elF-4E, blocking the formation of the cap-dependent mRNA translation initiation complex and suppressing translation. When 4E-BP1 is phosphorylated, elF-4E is released, and the initiation complex can form and promote translation [26]. Several studies have implicated components of the protein initiation synthesis apparatus in carcinogenesis. For example, elF-4E was shown to induce malignant transformation when overexpressed in mammalian cells [27]. Moreover, increased levels of elF-4E are commonly found in breast, prostate, and head and neck tumors, but not in benign lesions [28].
In our study, there was a significant positive correlation between mTOR and phos4E-BP1 expression as well as between mTOR and phosS6 expression in the bladder cancer cohort. Furthermore, phosS6 expression was elevated in bladder cancer cells compared with benign urothelium. PhosS6 expression was also significantly higher in high-grade bladder cancer cells. These results suggest that the mTOR pathway may contribute to the aggressiveness and progression of bladder cancer.
Among the mTOR pathway-related markers that we evaluated, phosS6 was a significant predictor of progression and DSS in the multivariate survival analysis, and phos4E-BP1 was a significant predictor of DSS. These findings are similar to those for other solid tumors; however, they are in contrast with prior studies that reported that phosS6 had a favorable prognostic effect in bladder cancer [25,29]. However, in the study by Schultz et al, 42% of the bladder cancer cohort underwent preoperative treatment including radiotherapy, systemic chemotherapy, or intravesical therapy [25]. Systemic chemotherapy and intravesical Bacillus Calmette Guerin (BCG) therapy may affect the expression of mTOR pathway-related markers as a result of telomerase activity and immune reactions [30,31]. In our study, therefore, we excluded patients with a history of preoperative treatment. Moreover, 49% of the bladder urothelial carcinoma cohort had a tumor staged higher than T3, whereas only 21% of the superficial bladder urothelial carcinoma cohort had a tumor at stage T3 or higher. A large proportion of patients with higher-stage bladder cancer may have a down-regulated mTOR pathway due to activation of HIF-1α. Additional large cohort studies are needed to determine the prognostic significance of mTOR pathway-related markers in bladder cancer patients.
In our study, strong phosS6 expression predicted shorter recurrence-free and progression-free survival in 145 patients with superficial bladder cancer who had undergone TURB, demonstrating that the mTOR pathway is involved in bladder cancer recurrence and progression. Moreover, these findings suggest that mTOR signaling may play a critical role in the progression and recurrence of superficial bladder cancer. Seager et al reported that rapamycin, an mTOR inhibitor, prevented progression of carcinoma in situ to invasive bladder cancer in an animal model [32]; furthermore, intravesical delivery of rapamycin into the bladder lumen was highly effective at suppressing bladder cancer recurrence. The risk of recurrence in patients with superficial bladder cancer treated with surgical resection alone ranges from 45% to 80% and in intravesical BCG it ranges from 46% to 69% based on 5- and 10-year follow-ups, respectively [1]. If currently available intravesical agents fail to eliminate the tumor, patients are faced with the prospect of radical cystectomy or urinary diversion. These are life-altering procedures fraught with significant metabolic and surgical complications, and the reluctance to accept these interventions hinges on the expected decrease in quality of life or comorbid medical conditions. Our findings suggest that superficial bladder cancer patients may be ideal candidates for testing mechanism-based targeted therapies in a clinical setting.
CONCLUSIONS
Our results revealed that mTOR pathway activation, as assessed by phos4E-BP1 phosphorylation, is involved in bladder cancer tumorigenesis and that S6 protein phosphorylation is a predictor of disease progression and poor cancer-specific survival. Moreover, we showed for the first time that S6 protein phosphorylation is related to high recurrence and disease progression in superficial bladder cancer patients. Trials designed to evaluate novel targeted agents in patients who are most likely to respond will accelerate the development of promising therapies. We hope that bladder cancer will rank highly among those human tumors to be effectively prevented and treated by "individualized" therapy.




 XML Download
XML Download