

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Neurofibromas of the penis are rare, but can involve the bladder, breasts in males, palatine tonsils, and colon or may be intercostal lesions [1-3]. Neurofibromas are often associated with neurofibromatosis type 1 (NF1) or Von Recklinghausen disease, and a plexiform neurofibroma of the penis associated with erectile dysfunction has been described [4]. Primary neurofibromas of the penis are extremely rare; to our knowledge, only about 20 patients with primary neurofibromas associated with penile neurofibromatosis have been described to date [4-8]. We describe here a patient with a solitary penile neurofibroma, without NF1, that was associated with erectile dysfunction.
CASE REPORT
A 37-year-old Korean man was referred to our hospital for evaluation of a solitary nodule on his penile shaft. He had been aware of a slow-growing, asymptomatic nodule for the previous 10 years. More recently, however, he experienced pain, tenderness, increased size, and difficulties during sexual intercourse and erectile dysfunction. His preoperative International Index of Erectile Function-5 score was 7.
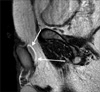
There was nothing notable in the patient's past medical history or family history, and he was generally in good health. A physical examination revealed a 2 cm-sized, ovoid, movable lesion on the dorsum of the penile shaft. The inguinal lymph node was not enlarged. He had no café au lait spots or auxiliary or inguinal freckling. An ophthalmologic examination revealed no glioma or iris (Lisch) nodules. The results of a complete blood count, electrolyte battery, liver function, renal function, and urine tests were all within normal limits. Magnetic resonance imaging (MRI) revealed a 2 cm-sized ovoid mass abutting the right corpus cavernosum (Fig. 1).
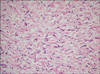
Local excision was performed with local anesthesia. The mass located between the corpus cavernosum and Buck's fascia was removed completely (Fig. 2). There was no neurovascular injury. The macroscopic appearance of the removed specimen was a 2 cm sized ovoid and bright reddish white mass such as a bean shape. Microscopic examination revealed spindle-shaped cells with wavy nuclei in fascicles (Fig. 3). Immunohistochemically, the cytoplasm of these cells was positive for S-100 protein (Fig. 4) and the vessels were positive for CD34. These results were consistent with a neurofibroma. After surgery, he had no pain, a normal sensation of the penile glans, and his erectile dysfunction had improved. At the present time, 26 months after surgery, the patient has experienced no signs of symptoms or recurrence.
DISCUSSION
NF1 is much more uncommon in the genitourinary tract than in other systems, with the bladder being the most commonly involved organ of the genitourinary tract [1]. Only one patient with primary neurofibromas associated with penile neurofibromatosis has been described to date in Korea [6]. Neurofibromatosis typically presents as genital masses or edema in males and clitoral hypertrophy, mimicking intersex condition, in females [9].
Although a penile neurofibroma involves continuity of the dorsal neurovascular bundle with the mass, the latter can be excised completely and safely, while preserving the dorsal bundle [4,10]. Although partial excision may be successful, complete resection is necessary not only for cosmetic and functional reasons but also to prevent recurrent problems and to prevent malignant degeneration [5]. Therefore, optimal timing of surgery is necessary to allow complete resection without organ impairment [7]. In our patient, the mass did not involve the dorsal neurovascular bundle and could therefore be resected.
Compromised penile function is caused by two major mechanisms. Difficulties in sexual intercourse may include an inability to penetrate due to the mass, despite experiencing normal sensation and erection, as well as erectile dysfunction, due to arterial stealing by the neurofibroma. A bilateral selective pudendal arteriogram showed that both arteries were hypertrophied and supplied the neurofibroma [4,7]. Thus, the erectile dysfunction in our patient was probably caused by a mass effect and psychological influence. The mass effect resulted in pain during sexual intercourse despite normal penile sensation. The patient gradually became more reluctant to have sexual intercourse and expressed low levels of self-esteem. After surgery, all his symptoms improved and there was no evidence of recurrence. In patients with functional impairment of the penis, resection of the lesion is associated with good outcomes.


 XML Download
XML Download