

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Guided by levels of prostate-specific antigen (PSA), prostate biopsy by transrectal ultrasonography (TRUS) has become a standard method in diagnosing cancer. TRUS-guided prostate biopsy is relatively safe and is usually well tolerated by patients. However, minor complications such as hematuria (13-58%), hematospermia (5-45%), or rectal hemorrhage (2-37%) or, rarely, major complications such as sepsis (0.1-2.2%), urinary tract infection with fever (1.4-4.5%), and urinary retention (0.2-2.6%) have been observed [1-7]. This case reports the first case of miliary tuberculosis (TB) occurring as a complication of prostate biopsy and emphasizes the possibility of this occurrence if the patient suffers from prostate TB.
CASE REPORT
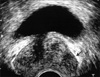
A 75-year-old man underwent TRUS-guided prostate biopsy because of a high serum PSA level (PSA: 13.104 ng/ml) detected during an examination for difficult urination. His medical history revealed pneumoconiosis, which was conservatively followed in the outpatient department of respiratory medicine. Urinalysis before the biopsy showed 1 to 4 red blood cells and 1 to 4 white blood cells per high-power field in the sediments. He was given prophylactic antibiotics (cefdinir 300 mg/day starting from 1 day before the biopsy for a total of 2 days and intravenous cefmetazole sodium 1 g during the procedure) before the TRUS-guided prostate biopsy. A hard mass without tenderness was palpable in the left lobe of the prostate by digital rectal examination (DRE). Physical examination of the scrotal contents revealed no abnormal findings. The TRUS findings revealed a prostate volume of 25 ml and a 12×16 mm hypoechoic lesion in the left peripheral zone of the prostate (Fig. 1). A fever spike over 38.5℃ began about 18 hours after the biopsy. The case was diagnosed as sepsis due to complication from the TRUS-guided prostate biopsy. He received antimicrobial treatment (intravenous piperacillin sodium 2 g, two times daily) for 5 days. However, the fever spike did not improve, and he began to cough 4 days after the biopsy. His white blood cell count was 5,200/mm3, with 85.5% neutrophils, 0.2% basophils, 10.7% lymphocytes, and 3.6% monocytes. C-reactive protein was 13.7 mg/dl. Blood and urine cultures were negative for pathogens. A chest computed tomography scan showed multiple nodular and macular shadows with pleural effusions in bilateral lungs, raising a suspicion of miliary TB (Fig. 2).
Polymerase chain reaction analyses for TB were positive in sputum, gastric washing, and urine, and sputum study was negative for Gaffky. The histopathological examination revealed TB of the prostate in 4 of 8 biopsy specimens (Fig. 3). By use of the Ziehl-Neelsen stain, acid-fast bacilli were detected in the midst of caseous necrosis. Initial treatment for 2 months consisted of rifampicin, isoniazid (INH), pyrazinamide, and ethambutol, and additional treatment for 7 months consisted of rifampicin and INH. The patient was discharged from the hospital 47 days after the prostate biopsy. It was uncertain whether the patient had actually suffered from pulmonary TB in the past. A follow-up transrectal prostate biopsy was not performed. The patient is now symptom-free, and the follow-up DRE revealed that the prostate had a smooth surface and ruby consistency 1 year after the biopsy. The post-treatment PSA level was 5.023 ng/ml.
DISCUSSION
Miliary TB was diagnosed in our patient resulting from the hematogenous spread following TRUS-guided prostate biopsy. The histopathological examination of the prostate biopsy revealed TB with acid-fast bacilli. Predicting prostate TB is very difficult because of its rarity. In a number of reported cases, it was diagnosed incidentally by the pathologist after a transurethral resection [8]. The clinical characteristics of prostate TB are usually nonspecific. Its main presenting symptoms are scrotal lesions, followed by lower urinary tract symptoms and painless gross hematuria. DRE findings are similar to those in prostate cancer, and the TRUS findings of diffuse hypoechoic lesions within the peripheral zone of the prostate frequently make it difficult to differentiate prostate TB from adenocarcinoma of the prostate. In the present case, a TRUS-guided prostate biopsy was performed because of the high serum PSA levels in our patient. In 18 patients with prostate TB, the median PSA level was 2.7 ng/ml (range, 0.3-31 ng/ml). The PSA level was greater than 4.0 ng/ml in 6 patients (33.3%) [9], which suggests that the PSA level might increase owing to the inflammatory reaction of TB. Thus, the diagnosis can only be confirmed by a prostate biopsy.
TB of the prostate is almost always the result of one or perhaps successive hematogenous seedings [10]. The primary site for infection of the genital tract is often the epididymis by hematogenous spread [8]. Lee et al reported that 50% of prostate TB is associated with TB of the epididymis. This suggested that the etiology and pathophysiology of these two diseases may be identical or directly related [9]. Physical examination of the scrotal contents might be useful for determining the possibility of prostate TB before the prostate biopsy with precise medical examination by interview. In addition, it seems that prostate TB should be considered in the differential diagnosis of prostate cancer because of the increased numbers of patients with human immunodeficiency virus (HIV) or other immunocompromised patients. Pneumoconiosis and advanced age were risk factors for developing miliary TB in our patient. This case is presented to acknowledge the possibility that miliary TB can occur as a complication of prostate biopsy if the patient suffers from prostate TB.


 XML Download
XML Download