

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The gold standard for the surgical treatment of clinically organ-confined prostate cancer has traditionally been open radical prostatectomy (RP). With recent advances in the laparoscopic approach as a minimally invasive procedure in a wide variety of surgical fields, laparoscopic radical prostatectomy (LRP) has been widely performed since 1997 [1,2]. Reported data in Western countries have shown that LRP results are comparable to those of open RP in terms of operative parameters, morbidity, urinary function, sexual function, and oncologic outcome [3-6]. Two main surgical approaches are used for RP in everyday urologic practice (transperitoneal and extraperitoneal). Extraperitoneal LRP (ELRP) allows direct access to the retropubic space, avoiding potential bowel injury, and it represents the technique that best replicates standard RP. Erdogru et al reported that there was no statistical difference in mean operative time (OT), complication rates, or positive surgical margins (PSMs) between the transperitoneal and extraperitoneal approaches [7].
To date, several studies have identified factors predicting the surgical outcome of patients with clinically localized prostate cancer who underwent open RP. Patient-related factors, such as obesity and prostate volume, have significant effects on the performance of open RP and robot-assisted laparoscopic radical prostatectomy (RALP) [8-13]. Direct access to the prostate during open surgery is limited by the overlying pubic bone. This anatomical challenge includes a deeper and possibly narrowed true pelvis, combined with occasional exostosis of the pubic symphysis. Although these challenges may hinder the surgeon's ability to operate efficiently and accurately within the laparoscopic field, LRP has potential advantages, such as magnified vision and reduced blood loss, that allow more precise dissection and reconstruction compared with open RP. Thus, we determined the effect of pelvic shape and pelvic arch interference, as shown on preoperative prostate magnetic resonance imaging (MRI), on the OT, estimated blood loss (EBL), and PSMs in patients who underwent ELRP.
MATERIALS AND METHODS
1. Patients
The study population consisted of 115 consecutive patients who underwent surgery performed by one surgeon between March 2006 and May 2009. We investigated various clinicopathologic variables, including age, body mass index (BMI), preoperative prostate-specific antigen (PSA) level, prostate volume (as measured by transrectal ultrasonography [TRUS]), pathologic stage, pathologic Gleason score, OT, EBL, and surgical margin status.
2. Estimated pelvimetry
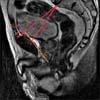
On the basis of the preoperative prostate MRI performed on a 3.0-T MR system (Magnetom Tim Trio; SIEMENS, Erlangen, Germany) with an 8-channel body coil, various bony pelvic dimensions likely to reflect the pelvic inlet diameter or depth were measured as follows (Fig. 1): the true conjugate diameter (the distance from the most superior aspect of the pubic symphysis to the sacral promontory) as measured on a midsagittal image from the MRI, the obstetric conjugate diameter (the closest distance from the pubic symphysis to the sacral promontory), and the difference between the true conjugate and the obstetric conjugate. This difference was intended to evaluate the extent of protrusion of the pubic symphysis. To assess the pelvic depth, we designated a new parameter, defined as the closest distance from the true conjugate to the apex of the prostate (pelvic depth), as measured on the midsagittal image from the MRI (Fig. 1).
3. Statistical analysis
Multiple linear and logistic regression analyses were used to identify associative factors for OT, EBL, and PSMs. All analyses were performed by using the SPSS ver 12.0 (SPSS Inc., Chicago, IL, USA). The results were considered statistically significant when the p-value was <0.05.
RESULTS
1. Patient characteristics
The mean patient age was 64.2±6.2 years, and the patients' mean BMI was 24.1±2.4 kg/m2. The mean preoperative serum PSA level was 14.7±21.2 ng/ml, and the mean prostate volume was 36.5±18.7 cc (Table 1).
2. MRI pelvimetry
The mean bony pelvic dimensions, as assessed on MRI, were as follows: true conjugate diameter, 112.1±10.7 mm; obstetric conjugate diameter, 99.3±7.2 mm; and the difference between the true conjugate diameter and the obstetric conjugate diameter, 12.7±3.7 mm. For the newly developed parameter of pelvic depth, the mean was 59.9±6.0 mm (Table 1).
3. Surgical outcomes
The OT was 260.1±91.1 minutes. The EBL was 633.3±524.7 ml. The PSM rate was 19%. The overall pathologic results showed clinically localized disease (pT2) in 68% of the patients and extraprostatic disease (pT3 or pT4) in 30% of the patients. The percentage of men with a pathologic Gleason score of ≤6, 7, and ≥8 was 25%, 56%, and 19%, respectively (Table 1).
4. Factors affecting OT, EBL, and PSMs
According to the multiple linear regression analysis, the prostate volume and pelvic depth were independent predictive factors for EBL (p=0.01 and p=0.01, respectively) (Table 2). The EBL rate was increased 3% (19.5/633.3x100) and 1.5% (9.6/633.3x100) as the pelvic depth was 1 mm deeper and the prostate was 1 cc larger, respectively. Factors that were correlated with a longer OT included the serum PSA, prostate volume, pelvic depth, and a Gleason score ≥8 (p=0.04, p=0.02, p=0.04, and p=0.001, respectively) (Table 3). According to the multiple logistic regression analysis, only pT2 was an independent factor of PSMs (adjusted odds ratio [OR], 3.9; 95% confidence interval [CI], 1.3-11.7; p=0.02) (Table 4).
DISCUSSION
It was recently reported that the oncologic results of ELRP are similar to those of open RP and transperitoneal LRP (TLRP) [14-16]. However, LRP is a difficult procedure that requires surgical skill and has a flat learning curve [4,17]. The outcomes of LRP depend on several factors, including surgical skill and the experience of the surgeon and the surgical team. In addition to the technical difficulties of the surgery, the body habitus of the patients can sometimes be an obstacle to any RP. Specifically, because an apical dissection is expected to be more challenging with a prostate lenges of an apical dissection are potentially more easily overcome with LRP than open RP, we sought to determine the effect of pelvic arch interference and the depth of the pelvic cavity on operative outcomes of LRP.
Several researchers have reported that obesity can make open RP more technically difficult. Chang et al identified BMI as a predictor of blood loss and transfusion during open RP [9]. Brown et al noted that there is a trend toward a longer OT in obese men undergoing LRP [18]. Even for RALP, Ahlering et al revealed that BMI significantly affects the OT and EBL [12]. Moreover, Castle et al reported a significantly higher rate of PSM and a significantly longer OT and increased EBL in obese patients who underwent RALP [19]. However, our results suggest that obesity does not have a significant effect on the results of LRP when the procedure is performed by an experienced surgeon.
Along with obesity, a large prostate is usually accompanied by increased vascularity and has been acknowledged by some surgeons as having significant effects on open RP or LRP. Hsu et al reported a direct correlation between blood loss, transfusion requirements, and prostate volume during open RP [8]. Patients with larger prostates had a transfusion rate 2.5 times that of patients with smaller prostates. Rassweiler et al noted a direct correlation between blood transfusion and prostate size during LRP; 17% of patients with a prostate <25 cc required transfusions compared with 47% of patients with prostates >45 cc [20]. Also, larger prostate volumes have been reported to be correlated with increased OT in most LRP studies [20-22]. Additionally, in several open or minimally invasive RP series, prostate volume was reported to have an inverse relationship with PSM rates [8,21]. In the current study, prostate volume was an independent predictor of OT and EBL, but not PSMs.
Similar to prostate volume, the dimensions of the pelvic inlet are an important parameter in predicting operative results. A large, wide pelvis allows increased operative movement and instruments to reach a large prostate. On the other hand, a deep, narrow pelvis and protrusion of the pubic symphysis tend to preclude the path of the laparoscope. Given that prediction of a difficult prostate apical dissection is important in reducing PSMs during LRP, it is necessary to have a better understanding of pelvic anatomical structure. If the working instruments are displaced out of the pelvis by pubic protrusion, the instruments may not reach the desired points during apical dissection or urethrovesical anastomosis.
An impression of pelvic size and shape may be gained from the patient's height, weight, and build, but such an impression is subjective, inaccurate, and will vary between urologists. Also, relevant objective data are sparse for bony pelvic dimensions on RP; therefore, pelvic size is difficult to quantify objectively. Kim et al previously developed new parameters for pelvic dimensions in an open RP study [23]. These parameters included views on MRI pelvimetry, which may provide a more reliable measurement of complex female pelvic floor structures than does X-ray pelvimetry, insights into the contribution of dystocia to obstructed labor in obstetric practice, and information for preoperative clinical staging of prostate cancer.
Therefore, using prostate MRI, we determined the amount of protrusion of the pubic symphysis from the pelvic cavity by applying obstetric pelvimetry and tried to objectify the pelvic depth from the pelvic inlet by using the distance between the pelvic inlet and the apex of the prostate. We determined the difference between the true conjugate diameter and the obstetric conjugate diameter. As the difference between the distances increased, the pubic symphysis protruding out of the pelvic cavity became longer. However, the amount of protrusion of the pubic symphysis from the pelvic cavity did not affect the surgical outcome. During open RP, the protrusion of the pubic symphysis affects the surgical outcome by narrowing the operative field and making the use of surgical instruments difficult, whereas the penetration of the laparoscope into the extraperitoneal cavity inside the pelvis was not affected. Therefore, the ease of securing the field of vision and the use of long micro-tools allow the surgeon to overcome the protrusion of the pubic symphysis.
Prostate volume and pelvic depth did affect the EBL and OT. That is, as the prostate volume increased by 1 cc, the EBL and OT increased by 9.6 ml and 1.2 minutes, respectively, and as the distance to the prostate apex increased by 1 mm, the EBL and OT increased by 19.5 ml and 2.8 minutes, respectively. Also, the preoperative PSA and a Gleason score ≥8 were had an effect on the OT.
Several studies have evaluated operative difficulty by using permutation of pelvimetry. Hong et al used preoperative MRI to determine the pelvic interspinous diameter (ISD), which reflects the pelvic area during open RP [24]. They analyzed the craniocaudal distance from the most proximal margin of the pubic symphysis to the distal margin of the apex of the prostate, designated the distance as apical depth (AD), and created a new parameter called the pelvic dimension index (PDI), which is the value of the ISD divided by the AD. However, this parameter does not affect EBL or OT [24]. Furthermore, they measured the anteroposterior diameter of the pelvic inlet (API; the distance from the most superior aspect of the pubic symphysis to the sacral promontory), pelvic depth (PD; the distance from the sacral promontory to the lower inner pubic symphysis), and the pelvic cavity index (PCI=API × ISD/PD) and applied it during RALP, but it had no effect on the operative result [25].
Emerson et al reported that a high preoperative PSA level was related to the rate of PSMs after open RP [26]. In our study, only pT2 was related to the rate of PSMs.
This study was not without limitations, including its retrospective nature, small number of cases, and consideration of only the preoperative factors affecting perioperative outcomes, but not surgeon's characteristics or surgical factors such as neurovascular bundle preservation, vesicourethral anastomosis, and pelvic lymphadenectomy. However, to minimize the confounding effect of surgical skill and technique, we confined our study to a single, experienced surgeon. Also, we used obstetric pelvimetry, which is a more physiologic parameter because of the movement of the fetal head during delivery. These are several factors that make our results different from other results.
CONCLUSIONS
The depth of the pelvic cavity and prostate volume evaluated by pelvic MRI are predictive factors for surgical difficulty during LRP. This can be considered useful information when planning LRP for clinically localized prostate cancer. However, further studies are warranted that include surgeon-related factors and surgical factors affecting the surgical outcome of LRP.




 XML Download
XML Download