

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Guidelines from the European Association of Urology (EAU) for the treatment of renal stones recommend extracorporeal shock wave lithotripsy (ESWL) and percutaneous nephrolithotomy (PCNL) as the standard therapies. ESWL is recommended as the therapy of first choice for renal stones <20 mm, and the success rate is approximately 90% [1]. However, the success rate of ESWL depends on the size, number, location, and hardness of the stones, and because of common residual fragments and the necessity for repeat procedures, there is concern over the use of ESWL for the treatment of large stones. Actually, ESWL for the treatment of large stones >20 mm has a reported stone-free rate of 45% to 60% [2-4]. Also, a limitation of ESWL for the treatment of lower calyceal stones can be found in studies that reported a low stone-free rate of 37% to 59% [5,6].
Due to its high stone-free rates, PCNL is the standard treatment modality for large stones >20 mm, staghorn stones, calyceal diverticular stones, or stones in the lower pole [1]. Although the stone-free rate following PCNL is between 78% and 95%, significant complications may be associated with the procedure, including urinary extravasation, transfusion, and fever. Major complications, such as sepsis, colonic injury, and pleural injury, are even more rare but still a source for concern [7,8].
In 1990, indications for retrograde ureteroscopic techniques were broadened to include intrarenal stones [9]. With improvements to endoscopic instruments and techniques, retrograde intrarenal surgery (RIRS) using ureteroscopy and laser lithotripsy for the treatment of renal stones is being used as a minimally invasive treatment modality, and a wide range of stone-free rates, from 50% to 94.2%, has been reported for this procedure [10-13]. RIRS may offer an alternative to ESWL or PCNL; however, to date, good scientific evidence is lacking to support the efficacy of this modality, which is not recommended as a first-line treatment for renal stones [1].
In this study, we reviewed our experience and evaluated the efficacy and safety of RIRS for the treatment of renal stones. In addition, we analyzed factors that will enable us to predict a stone-free result after surgery.
MATERIALS AND METHODS
We retrospectively reviewed the medical records and radiologic films of 83 patients who underwent retrograde intrarenal surgery for the treatment of renal calculi from January 2000 to July 2009. Patients with calyceal diverticular stones or medullary sponge kidney were excluded from the analysis. Preoperative imaging studies, including abdominal plain x-rays, intravenous pyelograms, or abdominal computed tomography (CT), were evaluated for characteristics of renal stones, including laterality, location, number, size, and radio-opacity. Locations of stones were subdivided into two groups: (i) the upper pole or midpole or renal pelvis and (ii) the lower pole with or without others. Stone size was calculated as cumulative stone burden. Stone burden was defined as the two-dimensional area determined by multiplying the longest diameter by the perpendicular diameter of the stone [14]. In cases of multiple stones, the total stone burden (cumulative stone burden) was calculated as the sum of the burden of each stone. Renal stones with irregular shapes such as staghorn stones were divided into several subunits, and the burdens of each of the units were summed. Cumulative stone burden was classified as 150 mm2 or less and greater than 150 mm2. Indications of RIRS were categorized into primary therapy without previous stone management and secondary RIRS with failed ESWL or failed PCNL.
All surgery was performed with the patient in the dorsal lithotomy position under general anesthesia. A safety hydrophilic guidewire was positioned in the upper urinary tract by use of 8/8.9 Fr. semi-rigid ureteroscopy and the patient underwent retrograde pyelography by fluoroscopy with contrast dye to identify urinary stones and the urinary tract. Except for renal stones, which could be accessed by use of semi-rigid ureteroscope only, a flexible ureteroscope was used (Karl Storz, Flex-X™ or Flex-X2™). A ureteral access sheath was placed according to the surgeon's preference. Stone fragmentation was performed with a Holmium-YAG laser using 200 or 365 µ fiber. Fragmented stones were extracted by using a stone basket or irrigation. For evaluation of stone clearance, the entire collecting system was inspected by means of flexible ureteroscopy; and fluoroscopic examination with or without contrast dye was performed to identify the presence of radio-opaque lesions or filling defects at the end of the procedure. A double J ureteral stent was routinely indwelled at the end of each procedure in all patients and was removed 2 weeks later on an outpatient basis. Postoperative follow-up radiographic studies including plain x-rays or CT scan were obtained at 1 day and 1 month after surgery.
Primary outcomes were the immediate and postoperative 1-month stone-free or success rate. We defined stone-free status as the absence of fragments on postoperative images and defined success as clinically insignificant residual stones less than 3 mm on postoperative images. Secondary outcomes were complications of surgery, and the predictive factors for a successful immediate postoperative stone-free rate.
In the univariate analysis, the statistical significance of indications for surgery and variables associated with stone characteristics (location, size, and number, etc) in relation to the immediate postoperative stone-free rate of RIRS were evaluated by using the chi-square test. Furthermore, multivariate analysis with logistic regression was performed for identification of the combined influences of these variables. Data were analyzed by using standard statistical software, SPSS ver. 17.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
Sixty-three patients with renal stones underwent RIRS; 3 of them had bilateral renal stones. Thus, a total of 66 RIRS cases were identified in the retrospective analysis. Table 1 lists patient demographics and the baseline characteristics of the renal stones. Patient age ranged from 51 years (range, 20-81 years), and there were 35 males and 28 females. Of 66 cases, 18 stones (27.3%) were located in the upper pole or midpole or renal pelvis and 48 (72.7%) stones were located in the lower pole with or without others, respectively. The mean cumulative stone burden was 168.9±392.5 mm2, with 49 cases (74.2%) of ≤150 mm2 and 17 cases (25.8%) of >150 mm2. Forty-one kidneys (62.1%) had a single or 2 renal stones and 25 (37.9%) had no fewer than 3 renal stones. Fifty-nine cases (89.4%) had radio-opaque stones and 24 (36.4%) were combined with ureteral stones.
Of 66 cases, RIRS was performed as the primary treatment for renal stones in 30 cases (45.5%) and as a second- line therapy after failure of primary ESWL or PCNL in 36 cases (54.5%). The most common indication for treatment was failure of ESWL (48.5%), followed by coexisting renal and ureteral stones (19.7%). Six patients (9.1%) had anomalies of the urinary tract, including 3 ureteropelvic junction obstructions, 2 horseshoe kidneys, and 1 ectopic kidney (Table 2).
A semi-rigid ureteroscope was used alone in 9 cases, and a flexible ureteroscope was used in 57 cases with 39 Flex-X™ and 18 Flex-X2™. The median operation time (calculated from the time of ureteroscope insertion to completion of stent placement) was 80 minutes (range, 30-250 minutes).
The immediate postoperative stone-free rate (SFR) was 69.7% (46/66) and increased up to 72.7% (48/66) at 1 month after surgery. The success rate was 80.3% (53/66) both immediately after the operation and 1 month later. Of 13 renal units with failed RIRS, 2 did not need any ancillary procedure due to clinically insignificant residual stones. Nine renal units underwent ancillary procedures, including 8 ESWLs and 1 PCNL, and the results from 3 showed residual stones ≤3 mm. Two patients were lost to follow-up.
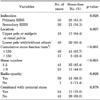
Immediate postoperative SFRs according to the variables analyzed are listed in Table 3. The SFR was significantly higher in primary RIRS than in secondary RIRS (83.3% vs. 58.3%, p<0.05). SFRs according to stone location were 94.4% for renal stones that were located in the upper pole or midpole or renal pelvis and 60.4% for those located in the lower pole with or without others, respectively (p<0.05). When stone locations were subdivided into 3 groups, including the upper pole or midpole or renal pelvis, the lower pole only, and the lower pole with others, the SFRs of each group were 94.4% (17/18), 73.3% (22/30), and 38.9% (7/18), respectively (Fig. 1). Renal stones with a cumulative stone burden ≤150 mm2 and a stone number of 1 to 2 stones presented a significantly higher SFR (p<0.05). No significant correlation between the SFR and radio-opacity or the presence of combined ureteral stones was found. Multivariate analysis of these factors showed that stone location and cumulative stone burden remained significant predictive factors of the immediate postoperative SFR (OR: 19.05 and 33.05, p<0.05) (Table 4).
No major intraoperative or postoperative complications were observed in any of the patients. There were 4 minor complications (6%), including 1 case (1.5%) of intraoperative minor ureter injury, which healed after transient ureteral stent indwelling; 2 cases (3%) of febrile urinary tract infection; and 1 case (1.5%) of postoperative paralytic ileus. None of the patients had transfusion or subcapsular hematoma. The median hospital stay was 3 days (range, 1-15 days).
DISCUSSION
EUA guidelines on the management of renal stones recommend ESWL as the first-line treatment for stones less than 20 mm and PCNL for stones more than 20 mm [1]. However, due to significant complications and clinical factors that influence treatment outcome, such as stone characteristics, anatomical details, and patient factors, there are limitations to the application of these recommendations to real practice. These perspectives have driven interest in other treatment modalities for renal stones, and, recently, RIRS, which may offer an alternative to ESWL or PCNL [1]. With the improvements to endoscopic instruments and techniques, the use of RIRS with flexible ureteroscopy and laser lithotripsy for the treatment of renal stones has increased. However, SFRs have been reported variably from 50% to 94.2% [10-13,15-17], and there are few reports in the literature on predictive factors for becoming stone-free.
Our study demonstrated that RIRS was an effective treatment for selective patients with renal stones. The immediate postoperative SFR was 69.7%, and the success rate including clinically insignificant residual fragments was 80.3%. Stone location and cumulative stone burden were significant predictive factors for the immediate postoperative SFR, and we found that SFRs of RIRS were particularly high for renal stones with a small burden, except for stones in the lower pole calyx. Also, RIRS could be performed safely with low minor complication rates (6%).
Stone location is an important factor that affects treatment outcomes for renal stones. Although ESWL for renal stones <20 mm has a high success rate of about 90% [1], SFRs for stones located in the lower pole decrease to 37% to 59% [5,6] and decrease to 55% for stones in multiple locations [18]. Because the SFR of ESWL in these stones was poor, PCNL was recommended for complex stones and lower pole stones greater than 10 mm [1,6,7]. However, PCNL has a risk of significant complications such as renal parenchyma injury, bleeding, urine leakage, postoperative pain, and long hospitalization [7,8,19,20].
Advances in distal tip deflection and scope durability of the flexible ureteroscope allow access to and treatment of stones throughout the intrarenal calyceal system [16]. Perlmutter et al studied the impact of stone location on the success rate of RIRS for the treatment of renal stones ≤20 mm [13]. They reported SFRs of 100% for upper pole stones, 95.8% for midpole stones, and 90.9% for lower-pole stones and concluded that stone location did not significantly affect the SFR. In contrast, Pearle et al reported a low SFR of 50% for RIRS and found no significant difference with the SFR of ESWL of 35% in their prospective and randomized trial comparing ESWL and RIRS for lower pole stones sized 10 mm or less [10]. Meanwhile, when patients with multiple unilateral renal stones underwent RIRS, Breda et al demonstrated that SFRs after 1 and 2 procedures were 64.7% and 92.2%, respectively [16].
In the present study, we subdivided stone locations into two groups: stones in the upper pole or midpole or renal pelvis and stones in the lower pole with or without others. The SFR differed significantly between the two groups: 94.4% and 60.4%, respectively. Stone location was also an independent predictive factor of the SFR in the multivariate analysis. When stone locations were again subdivided into three groups, including the upper pole or midpole or renal pelvis, the lower pole only, and the lower pole with others, the SFRs of each group were 94.4%, 73.3%, and 38.9%, respectively. The SFRs for patients with stones located in calyces, except for those in the lower pole or lower pole only, were similar to those reported in previous studies [13,15]; however, SFRs were particularly low in cases of multiple calyceal stones in the lower pole. This low SFR may be affected by the larger size and multiple numbers of stones.
We can conclude for certain that stone size is a powerful factor in predicting the SFR for RIRS. In our series, the SFR for stones with a cumulative stone burden ≤150 mm2 was significantly higher than that for stones with a cumulative stone burden >150 mm2 (83.7% vs. 29.4%). Our study supports the EAU guidelines stating that RIRS could become a reliable first-line treatment for lower pole stones ≤1.5 cm [1].
In this study, we categorized indications of RIRS into primary therapy (45.5%) as a first-line treatment and secondary therapy (54.5%) after failure of a previous treatment, mostly ESWL, and the immediate postoperative SFRs were 83.3% and 58.3%, respectively (p=0.028). The SFR of secondary RIRS was similar to the 46% to 67% SFR reported in a previous series of RIRS that was performed as second-line treatment for ESWL-resistant renal stones [21-23]. Stav et al and Jung et al mentioned that RIRS was a safe and effective procedure for ESWL-resistant renal stones; however, large stones and lower calyceal stones were negative factors that reduced RIRS success [21,22]. In a retrospective comparison of RIRS performed as the primary treatment and as a second-line therapy after ESWL failure [23], the authors reported that RIRS after failed ESWL has a significantly lower success rate than first-line RIRS (80% vs. 67%). They then suggested that careful consideration should be given to the best second-line therapy comparing RIRS with PCNL for patients with unfavorable lower-pole anatomy or previous multiple ESWL sessions.
In our series, secondary RIRS produced a lower SFR than did primary RIRS; however, the indication for surgery was not an independent factor for prediction of the SFR in the multivariate analysis. Indeed, most of the 36 cases that underwent RIRS as secondary therapy had larger stones (mean cumulative burden 225 mm2) and stones in multiple calyces with lower pole involvement (18 cases in lower pole only and 12 in lower pole with others), which are negative predictive factors. In these unfavorable patients with larger and multiple calyceal stones, the SFR of 58.3% could be an acceptable result; therefore, we suggest that RIRS as a second-line treatment is a useful treatment modality for ESWL-resistant renal stones.
The causes of failed RIRS in the present study were renal stones that were located in calyces with an acute infundibulopelvic angle or narrow infundibulum and intraoperative bleeding that could obstruct the operative field of vision. As mentioned in a recent study, pyelocaliceal anatomy, deflection of the endoscope, and loss of deflection after the insertion of instruments through the working channel could influence the success of the flexible ureteroscopic approach. These factors should be evaluated before recommending RIRS for the treatment of renal stones [24].
Although a limitation of the present study is its retrospective design, we suggest that our results may provide valuable data on predictive factors for successful RIRS. When considering RIRS for the clinical treatment of renal stones, these data may be useful indicators for determining the prognosis of treatment after RIRS.
CONCLUSIONS
RIRS is a safe and effective treatment for renal stones. The immediate postoperative SFR and success rate of the procedure were 69.7% and 80.3%, respectively, and the overall complication rate was 6%. The SFR of RIRS was particularly high for renal stones with a small burden, with the exception of those in the lower pole. RIRS should be considered as a primary treatment modality in selective patients with renal stones.




 XML Download
XML Download