

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Stress urinary incontinence (SUI) is a common chronic condition that affects women's quality of life. The synthetic, tension-free vaginal tape (TVT) procedure for the reinforcement of the midurethra was introduced in the 1990s as a surgical treatment for women with SUI. In 2001, a new minimally invasive procedure, the transobturator tape (TOT) technique, was developed and is associated with both simplicity and safety [1]. Even though follow-up for the TOT procedure is short, the procedure has been associated with the development of infectious complications [2], and different types of erosions because of foreign body reactions [3]. Here we report a case of a bilateral recurrent thigh abscess manifesting 5 years after a TOT sling procedure.
CASE REPORT
A 46-year-old woman presented to our emergency department complaining of increasing pain in her right thigh and groin for 1 week previously. Her right thigh was tender and swollen. Her past medical history was significant for a TOT procedure 5 years ago at a local clinic. She had been treated in the orthopedic department of another hospital two consecutive times in the past 1 year for recurrent bilateral thigh abscesses with repeated incisions and drainages. She had also undergone removal of the suburethral polypropylene mesh 5 months earlier in our hospital. However, at that time, complete removal of the mesh was impossible because pulling the right part resulted in snapping of the mesh because it had adhered to the tissue.
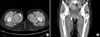
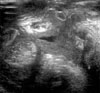
On the physical examination, the right medial thigh area was painful and tender on palpation. There was a 2×2 cm sized area of swelling that protruded approximately 0.5 cm. The patient's vital signs were normal, but urinalysis showed pyuria, and her C-reactive protein (CRP) was elevated. Computed tomography (CT) of the thigh was performed to determine an accurate size of the abscess. The CT showed an abscess located in between the adductor magnus and gracilis muscles, approximately 2.5×3×3 cm in size (Fig. 1). The mesh was not visualized on CT. The patient was admitted and received conservative management including intravenous antibiotics. On the fifth day of admission, she had a fever of up to 39.2℃ and chills, and aggravated groin pain with swelling in the right pubic area. Ultrasonography of the thigh on the sixth day showed an increased abscess pocket (longest axis, 6 cm) and severe muscular swelling (Fig. 2). Vaginal examination revealed the eroded remnant mesh with an abscess pocket. The patient underwent drainage of the abscess through a 1 cm incision in the pubic area. Approximately 150 cc of yellowish pus was drained, and the resulting culture grew Streptococcus (not group A, B, C, D, F, G). Together, through a 3 cm sagittal incision in the anterior vaginal wall under the midurethra, the remaining mesh was removed completely. At this time, when the exposed tip of the mesh was pulled, the remnant 5 cm of mesh was easily extruded and separated from the tissue with the abscess formation. The cavity was then washed out with iodine/povidone. A drain was inserted and removed after 48 hours, and the Foley catheter was removed before discharge on the seventh postoperative day. Two months after this operation, the wounds were observed to be closing and the patient has not had a recurrence of the infection or the SUI.
DISCUSSION
The TOT procedure has been noted to be the safest and most minimally invasive treatment of SUI because the insertion avoids the retropubic approach of TVT and, ultimately, the bladder, the gastrointestinal tract, and other major vessels. Therefore, complication rates such as bladder perforations, pelvic hematoma, and storage lower urinary tract symptoms following placement of the TOT are usually considered to be low and less common than with the TVT procedure [4]. In a study of 604 TOT patients, the reported incidences of bladder perforation, vaginal perforation, hemorrhage, and hematoma were 0.5%, 0.33%, 0.83%, and 0.33%, respectively [5]. However, because all synthetic slings are foreign bodies, different types of erosions and infections have been described. Marcus-Braun and von Theobald reported 104 mesh removals owing to various complications such as erosion, infection, pain, and shrinkage of the mesh over the course of 5 years among more than 1,200 vaginal mesh operations, which suggests an overall complication rate of less than 10% [6].
Thigh abscesses are a new infectious complication of suburethral sling surgery and can be explained by the anatomical route of the TOT along the obturator fossa. Other cases of thigh abscesses after TOT have been published that occurred within a few days after the operation [7] or up to 2 or 3 years postoperatively [8]. Our patient demonstrated that transobturator abscesses may manifest even 5 years after surgery. Although a thigh CT and ultrasonography were performed in this case to confirm the abscess, it is generally known that MRI is a more accurate diagnostic tool for assessing the extent of infection and the position of the tape [9].
In most cases, because tape erosion precedes abscess formation, careful vaginal inspection must be performed for patients with suspected thigh or obturator abscesses after TOT procedures. In the case of vaginal erosion only, resection of the protruding part and covering by use of the surrounding vaginal mucosa is usually performed. However, with repeat erosion, infection, malposition, pain, and mesh shrinkage, complete mesh removal is unavoidable. Deffieux et al reported on the removal of only the suburethral portion of an infected sling with a subsequent thigh abscess 9 months later, thus confirming the importance of complete removal of infected sling material [10]. Our case also experienced abscess recurrence 5 months after incomplete mesh removal, suggesting that removal of the entire tape is very important to prevent recurrences. Additionally, conservative management with intravenous antibiotics only is highly undesirable. Once there is known abscess formation, immediate incision and drainage of the abscess is recommended. After complete mesh removal, the patient may experience recurrence of incontinence. Marcus-Braun and von Theobald reported a 37.8% recurrence rate of SUI after partial or complete removal [6]. Fortunately, our patient has not yet had any recurrence of SUI.
In conclusion, this case demonstrates the necessity for any urologist treating women who have undergone TOT procedures to be aware of the possibility of abscesses.
 XML Download
XML Download