

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Urinary calculi disease is one of the most common urological disorders, with an incidence of approximately 0.1% to 0.3%. The lifetime prevalence is estimated to be about 5% to 10%, and the risk of stone recurrence in a 10-year period is approximately 74%. Stone disease typically affects adult men 3 times more commonly than adult women and shows a peak incidence in the fourth to sixth decades of life [1,2]. Currently, the treatment of patients with urolithiasis has been greatly changed with advances in minimally invasive techniques, the continued development of which has decreased morbidity with better efficacy. However, the recurrence rate of urinary stone disease is still high despite the successful removal of stones. There is no doubt that the prevention of stone recurrence is as important as treatment, and preventive measures should be made through metabolic evaluation that elucidates the underlying risk factors for stone formation.
The risk of stone disease is known to be correlated with various environmental factors such as climate, socioeconomic status, geography, dietary habits, and obesity [3,4]. Numerous reports have also noted genetic correlations such as sex, age, race, idiopathic hypercalciuria, hyperoxaluria, and hyperuricosuria [5-8]. Also, about 25% of patients with urolithiasis have a family history of stone disease, and the relative risk of stone formation is higher in men with a family history than in those without a family history [7]. In addition, pediatric patients with urolithiasis also have a positive family history in 46.2% of first-degree and 32.5% of second-degree relatives [9]. Generally, the familial affinity of urinary stone disease has been considered to be affected by environmental factors such as similar diet patterns among family members as well as genetic influence. However, the limited data make it difficult to clarify the potential interaction between family history and urolithiasis. Therefore, this study aimed to examine the influence of family history on urinary stone disease by comparison of clinical features and serum and urinary metabolic profiles according to the existence of a family history.
MATERIALS AND METHODS
We reviewed a database of 1,068 patients (715 males and 353 females) among 4,038 patients who were referred to our hospital for urolithiasis between March 1994 and February 2008. The patients had completed a metabolic evaluation including history taking and serum and 24-hour urinary examination. Among them, 192 (18%; 131 males and 61 females) had a family history, whereas 876 (82%; 584 males and 292 females) did not. Family history was defined as positive when any first-degree relative had an episode of stone disease; the cases who could not clearly remember were excluded. The exclusion criteria were as follows: patients with a bladder stone, infection stone, or abnormal urinary tract on radiologic exam; patients with other metabolic diseases (hyperparathyroidism, hyperthyroidism, chronic renal failure, hepatic cirrhosis, etc); and inappropriate urine collection.
Within 1 or 2 months after the completion of stone removal, we performed serum chemistry, urinalysis, and culture measurements and a 24-hour urinary metabolic evaluation with the patient on his or her usual diet without any medications. Twenty-four-hour urine specimens were collected by discarding the first urine sample right after waking up and collecting the following urine samples until the first urine on the next day in an exclusive bag with 3 cc toluene. The patients were instructed to turn in the collected urine within 2 hours. The urinary metabolic evaluation included urine volume, sodium, phosphorus, uric acid, calcium, oxalate, citrate, and pH. Given the 24-hour urinary creatinine level, the cases with less than 1.0 g in males and 0.8 g in females were excluded in the analysis as having an inappropriate collection. Urinary metabolic abnormalities were classified according to the definitions of Lifshitz et al [10].
Data analyses were performed by using SPSS Inc. (version 12.0, Chicago, USA). Clinical features, serum and urinary chemistry indexes, and urinary metabolic abnormalities were compared between the two groups. Student's t-test was used for continuous variables, such as serum and urinary chemistry indexes, and chi-square test for nominal variables, such as the frequency of urinary metabolic abnormalities. Statistical significance was set at a p-value of less than 0.05.
RESULTS
1. Comparisons of clinical characteristics
No differences were found in sex, age, or body mass index (BMI) between the groups (p>0.05, respectively). Although the group with a family history showed higher rates of episode and multiplicity of stones than did the group without a family history, these differences were not statistically significant (Table 1).
2. Comparisons of serum metabolites
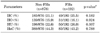
There were no statistically significant differences in serum phosphorus, uric acid, sodium, potassium, or creatinine values between the groups with and without a family history. However, a statistically significant difference was observed in the serum calcium level, with the group with a family history showing higher values (9.2±0.5 vs. 9.3±0.5, respectively, p=0.048) (Table 2).
3. Comparisons of 24-hour urinary metabolites
Results are shown in Table 3. The urinary excretions of phosphorus, uric acid, oxalate, and citrate did not differ significantly between the groups. Twenty-four-hour urine volume and pH were also similar. However, the urinary excretion of calcium was significantly higher in the group with a family history than in the group without a family history (p=0.042).
4. Comparisons of urinary metabolic abnormalities
When urinary metabolic abnormalities were compared between the groups, the frequency of hypercalciuria, hyperoxaluria, hyperuricosuria, and hypocitraturia did not differ significantly in any of the analyses (Table 4).
DISCUSSION
Although numerous studies have identified the risk factors for urolithiasis, the exact cause of stone formation is often unknown [5,9]. Hypercalciuria is the most important risk factor in calcium stone formation, occurring in 35% to 65% of cases. Urinary calcium raises the ionic calcium concentration and increases the urinary saturation of stone-forming calcium salts (calcium-phosphate or calcium-oxalate) [11,12]. In addition, complexation of calcium with urinary inhibitors such as citrate and glycosaminoglycans reduces urinary inhibitory activity, thereby increasing stone risk [13,14]. Although hypercalciuria can be accompanied by diseases causing a hypercalcemic state such as primary hyperparathyroidism, myelo-proliferative disease, vitamin D intoxication, or Cushing's syndrome, most hypercalciuria is idiopathic and results from hyper-absorption of calcium in the intestine or failure of calcium reabsorption in the renal tubule [11]. In addition, hypercalciuria may have a genetic predisposition, and about half of patients who have hypercalciuria have a family history of stone disease [15].
Recent studies have suggested a close relation between urolithiasis and family history [16,17]. Urolithiasis develops more frequently in individuals with a family history of kidney stones than in those without a family history, but little information is available regarding whether the increased risk is attributable to genetic factors, environmental exposures, or some combination. A positive family history of stones has been reported in 16% to 37% of patients who have formed a kidney stone, compared with 4% to 22% in healthy control subjects [7,18-20]. Previously, Curhan et al examined the association between family history and risk of kidney stone formation in a cohort of 37,999 male participants in the Health Professionals Follow-up Study [16]. In their study, kidney stone formers with family history had significantly higher urinary calcium excretion than did those without a family history. They also showed that a family history of kidney stones substantially increased the risk of stone formation. Of interest, Lerolle et al reported a significant dose-effect association between calciuria and stone disease in patients with familial hypercalciuria [17]. In the present study, we found that the serum calcium level and urinary calcium excretion were significantly higher in the group with a family history than in those without a family history. Additionally, our results support previous studies showing that a family history of urolithiasis is closely associated with an increased risk of urinary stone formation [16,17].
Uric acid is an end product of purine metabolism and functions as the nucleus of urinary crystallization to induce the formation of calcium oxalate stones. It is also responsible for urinary stone formation by reducing the activity of inhibitors in the urine [21]. Hyperuricosuria may also be related to a family history. This relation can be supported by the fact that the metabolism and excretion of uric acid may be influenced by inherited factors and that men with gouty diathesis are at increased risk of stone formation [22,23]. Curhan et al found increased urinary excretion of uric acid in a group with a family history of renal stones, but statistical significance was not reached [16]. Our results also revealed no significant difference between urolithiasis patients with and without a family history.
Urinary oxalate excretion has been thought to be important for urinary stone formation because a small change in urinary oxalate can cause a great change in urinary calcium-oxalate saturation. Although there are recognized genetic disorders resulting in an overproduction of oxalate, such disorders are very rare and the association between hyperoxaluria and a family history is still not evident [16].
Hypocitraturia is also known as an important risk factor for calcium oxalate stone formation [24-26]. However, studies on the relation of family history and hypocitraturia are scarce, and there has been no research since Curhan et al reported a significant increase in citrate excretion in patients with a family history [16]. In the present study, we did not find a significant relation between family history and hypocitraturia. In light of these results, therefore, it is unlikely that urinary citrate excretion is related to family history.
Although our data showed no statistical difference in the frequency of hypercalciuria (21.1% vs. 25.5%, p=0.182) between urolithiasis patients with and without a family history, we found that the patients with a family history had more elevated serum calcium concentrations and higher urinary excretion of calcium than did those without a family history. This finding suggests that hypercalciuria may be responsible for the familial characteristic of urolithiasis.
CONCLUSIONS
In this study, the urolithiasis patients with a family history showed higher serum calcium levels than did those without a family history and a tendency for increased excretion of urinary calcium. This result suggests that a family history of urolithiasis might be related to abnormalities in calcium metabolism.



 XML Download
XML Download