

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Open nephron-sparing surgery (NSS) is effective for the management of T1a (≤4 cm) renal cell carcinoma (RCC) [1,2]. Initially reserved for patients in whom preservation of renal function was needed with durable long-term success [3], NSS has been increasingly offered to patients with normal contralateral kidneys [4]. The widespread inclusion of laparoscopic partial nephrectomy (LPN) in the surgical armamentarium for the management of renal cancer, however, has evolved slowly because of technical difficulties related to the procedure [5].
Originally, LPN was restricted to small, exophytic, and peripheral tumors. With increasing experience, however, indications for LPN have expanded to more complex tumors, albeit in the hands of laparoscopic experts [6]. Current advances in laparoscopic surgery, such as knot-tying aids [7], hemostatic agents [8,9], intra-operative maneuvers [10], and newer laparoscopic instrumentation [11], have greatly helped to make this procedure technically feasible and reproducible by a wider range of surgeons. LPN is thus becoming a valid alternative when NSS is considered. In a European study, LPN provided results similar to open surgery [12]. We present the Korean experience comparing LPN with open NSS for the management of renal tumors.
MATERIALS AND METHODS
1. Patients
Between January 1998 and May 2009, 417 consecutive patients underwent LPN for the management of renal tumors by surgeons of 15 institutions in Korea. Of the 417 patients, 273 met the inclusion criteria of solitary, pathologic T1a tumors (≤4 cm) without a history of ipsilateral renal surgery. Thirty-nine patients underwent robot-assisted LPN. These patients were compared with a cohort of 279 patients who underwent open partial nephrectomy (OPN) performed by the same surgeons between January 1998 and May 2009; these patients also met the same inclusion criteria. The techniques used for both LPN and OPN have been previously described [7,13].
3. Peri-operative analysis and follow-up
Renal function was assessed by measurement of serum creatinine. To improve the accuracy of renal function determination, the glomerular filtration rate (GFR) was estimated using the Mayo Clinic Quadratic Equation (MCQE), thereby lowering the effect of underestimation of a high GFR compared to other estimation formulae [14]. Renal function was graded as suggested by the US National Kidney Foundation [15]. Complications were rated as intra- and post-operative and graded according to the National Cancer Institute Common Toxicity Criteria (NCI-CTC)-based grading system developed by Simmons and Gill [16]. Most of the patients were followed at each institution, with serum creatinine analysis, urinalysis, and renal imaging (mainly CT scans) at 6-month intervals for 3 years and thereafter at yearly intervals.
4. Statistical analysis
The stage of renal cell cancer was pT1 in all cases. The two groups were compared regarding surgical, clinical, and pathologic outcome variables. The Student's t test was applied for comparison of continuous variables. The Pearson chi-square test and Fisher's exact test were used to compare categorical variables. The five-year overall and recurrence-free survival (RFS) rates for local and distant relapse in pT1 stage RCC were estimated using the Kaplan-Meier method with log-rank test statistics. All analyses were performed using the Statistical Package for the Social Sciences (version 17; SPSS, Chicago, IL, USA), with a two-sided p-value<0.05 considered to indicate statistical significance.
RESULTS
The groups were similar with respect to age, gender, and body mass index (Table 1). The pre-operative creatinine level was similar in both groups. Despite matching for tumors <4 cm in size, a significant mean difference in tumor size existed between the OPN and LPN cohorts; however, it was only a 2 mm difference on average between the groups.
LPN was attempted to replicate the surgical technique of OPN with one exception. Eighty OPNs used cold ischemia, while all LPNs were performed with warm ischemia (WI). Other notable findings between the two procedures included a longer mean surgical time in the LPN group compared to the OPN group (221 min vs. 184 min, p<0.001) and a longer ischemia time (33.3 min vs. 23.4 min, p<0.001). The surgical and ischemic times of robot-assisted LPN were 245±92 min and 30.1±16.2 min, respectively, which were similar to non robot-assisted LPN (p=0.231 and p=0.078, respectively). LPNs were associated with less estimated blood loss (EBL; 293 ml vs. 418 ml, p<0.001). The mean length of follow-up of the OPN group was longer than the LPN group (28.0 months vs. 17.8 months, p<0.001).
The final pathology report revealed clear-cell carcinoma in 86.7% and 85.3% of the OPN and LPN patients, respectively (p=0.611). Twelve (4.4%) and 7 positive margins (2.5%) occurred in the LPN and OPN cohorts, respectively (p=0.161).
Open conversion was required in 2 patients (0.7%) in the LPN group because of intra-operative hemorrhage and radical nephrectomies were performed. Radical conversion occurred in 4 of the OPN patients (1.4%) due to intra-operative hemorrhage.
The overall incidence of intra-operative complications was similar in both arms (Table 2). The following three intra-operative complications occurred in the LPN patients: a spleen injury that was repaired laparoscopically and two open conversions secondary to hemorrhage. The total complications were similar in both cohorts (OPN, 6.8%; LPN, 6.6%; p=0.919). When complications were stratified, minor and major complications were similar between the two groups. The majority of these complications were pseudoaneurysms, which were repaired by angioembolization in five patients in both arms. Post-operative urine leakage developed in three patients who underwent OPNs; two of the patients were managed with prolonged Jackson-Pratt drainage, and the third patient needed percutaneous drains. Three patients with urinary leakage in the LPN cohort were treated conservatively with prolonged Jackson-Pratt drainage.
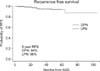
The short-term oncologic outcome and early recurrence were similar in both arms. Local recurrences were found in both groups (LPN, 0.7% [n=2]; OPN, 1.0% [n=3]); 0.7% (n=2) and 2.1% (n=6) of the patients developed distant metastases to the liver, cecum, lymph nodes, or pancreas after LPNs and OPNs, respectively. At 5 years, the Kaplan-Meier estimates for recurrence-free rates were 96% and 94% after LPNs and OPNs, respectively (p=0.332). Three and four patients died during follow-up after OPNs and LPNs, respectively, but other patients in both groups died due to other causes than RCC (Fig. 1).
The decline in post-operative GFR did not differ between the two groups (p=0.8) (Table 3). On multivariate regression analysis, pre-operative GFR and ischemia time independently predicted the post-operative GFR decline.
DISCUSSION
The principal findings of our Korean multicenter study were comparable surgical, oncologic, and functional outcomes after laparoscopic and open NSS. Shorter operative and hospitalization times following the laparoscopic approach reveal advantages in terms of reduced peri-operative morbidity, as well as non-urologic complications [17]. Previously, open NSS was reserved for patients with a solitary kidney or renal insufficiency. With complication rates and cancer control rates comparable to those for radical nephrectomies for tumors <4 cm in size, however, partial nephrectomy is now viewed as an acceptable alternative for many patients with renal masses [18]. Contrary to laparoscopic radical nephrectomy, LPN has been slow to become an alternative to open NSS; this is caused in large part by the very high level of technical expertise needed to perform the procedure [6].
Similar to the large multi-institutional series presented by Gill et al [19], blood loss was minimal while ischemia time was longer for LPNs. In our series, however, we did not find a greater rate of intra- or post-operative complications, as reported by Gill et al [19]. Their series had significantly more post-operative complications in the LPN group (24.9%, LPN; 19.2%, OPN), although the series presented by Schiff and coworkers [17] (9%, LPN; 19%, OPN) and our group (6.6%, LPN; 6.8%, OPN; p=0.919) found the opposite. This may be attributed to the small difference in mean tumor size and tumor location between Gill's series [19] and our series. Tumors in the OPN cohort, however, were on average only 5 mm larger than tumors in the LPN cohort in our series, which is less than that presented by Gill et al [19] (3.5 cm, OPN; 2.7 cm, LPN) and Schiff [17] (3.4 cm, OPN; 2.2 cm, LPN). Overall complication rates for LPN in the literature range from 6% to 33% and for OPN from 4.1% to 38.6% [12,20-22]. Our retrospective multicenter study did not regard blood transfusion due to hemorrhage as a post-operative complication because the indications for blood transfusion at each institution and for each physician were different. However, simply adding the transfusion rate to the complication rate for LPNs and OPNs yielded 16.1% and 23.6%, respectively; these results were similar to a previous Western study [20-22].
Also in our analysis, data on the oncologic outcome must be interpreted with caution because of the rather short follow-up. The Cleveland Clinic Foundation reported excellent results, with 100% distant and 97.3% local recurrence-free survivals within 5.7 years of LPNs [23]. Canes presented comparable 97.5% and 98.3% distant and local recurrence-free survival estimates, respectively, at 5 years for OPNs [24]. Similar data have been reported by others [21]. Our data suggest that open and laparoscopic access yield comparable oncologic efficacy in the treatment of pT1 stage RCC. The impact of positive margins on disease outcome has been discussed controversially. As we observed similar rates of positive surgical margins in LPNs and OPNs, it may be that the limited maneuverability of laparoscopic instruments does not significantly affect the accuracy of tumor excision. A multicenter analysis of LPNs showed positive margins in 1.8-2.4% of cases [24], and a slightly higher rate of 6.7% in solitary kidneys [25]. The positive surgical margin rate of OPNs is similar, with 7% in an analysis of 777 patients by Kwon et al [26]. The positive surgical margin rate of LPNs and OPNs was 4.4% and 2.5%, respectively, in the current study. It is important to understand that positive margin status does not necessarily indicate residual disease or translate into disease progression, as only 4% of patients with positive margins will eventually develop local recurrences [26]. Nevertheless, patients with positive surgical margins require close post-operative monitoring.
Marszalek et al reported that the decline in the GFR at the last available follow-up (LPN, 10.9%; OPN, 10.6%) was similar in both OPN and LPN groups (p=0.8) [12]. In the current study, the decline in renal function was similar after LPNs and OPNs despite a longer WIT in LPN patients. Based on a multivariate analysis, laparoscopic access was not an independent risk factor for GFR impairment in the post-operative phase. Pre-operative renal function was, besides ischemic time, one predictive factor for the long-term decline in GFR in our study. Our study did not show the beneficial effect of the robot system on ischemic time because robot-assisted LPN was in its infancy of use in Korean institutions for partial nephrectomies.
We acknowledge that the retrospective nature of the analysis is a shortcoming of this study. It was likely that complication rates were under-reported. Furthermore, non-identical protocols from multi-institutions might have reduced the statistical power in analysis so that some associations were not detected. Long-term follow-up is needed to verify long-term oncologic and functional outcomes.



 XML Download
XML Download