

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Although complete or incomplete ureteral duplication is one of the most common congenital malformations of the urinary tract, ureteral duplication with concomitant lower pole ureteropelvic junction obstruction (UPJO) is unusual, and the simultaneous presence of multiple renal stones is rare.
Until recently, the standard treatment of UPJO in a duplex renal system was open pyeloureterostomy. However, minimally invasive endoscopic surgery is preferred in selected patients. We describe our experience with the successful management of UPJO in a partially duplicated collecting system in both a retrograde and an antegrade fashion.
CASE REPORTS
Case report 1
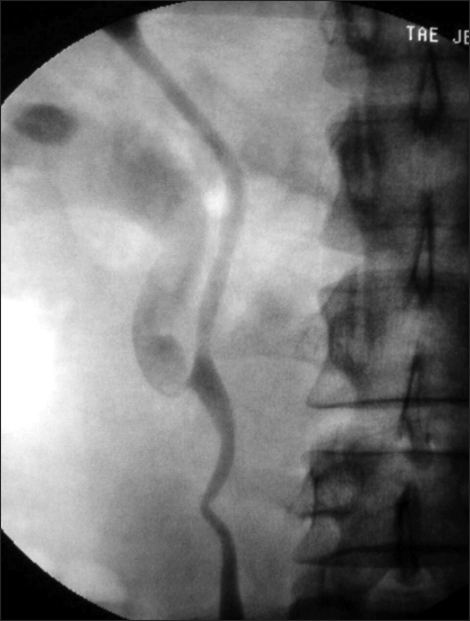
A 32-year-old man was referred with dull, aching right flank pain for 3 years. The patient was evaluated by abdominal computerized tomography, which revealed incomplete duplication of the right urinary system with lower pole moiety hydronephrosis. No extraluminal crossing vessels were detected. Retrograde pyelography showed UPJO with moderate hydronephrosis of the lower pole moiety (Fig. 1). An endopyelotomy with the Acucise® (Applied Medical) ureteral cutting balloon device was planned.
With the patient in the dorsal lithotomy position, a 0.038-inch guidewire was inserted into the lower pole of the collecting system, and an Acucise® cutting wire was pre-aligned in the posterolateral position. We introduced the Acucise® over the guide wire and advanced it just proximal to the UPJ stricture. Under C-arm fluoroscopy, the Acucise® Cautery balloon wire was used to incise the narrowed ureteropelvic junction in the posterolateral direction. The operative retrograde pyelography confirmed a successful incision of the narrowed ureter through extravasation of contrast medium. A 6 Fr stent was placed in the lower collecting system for 6 weeks. An intravenous pyelography at 3 months postoperatively showed marked reduction of the hydronephrosis in the lower pole moiety (Fig. 2).
Case report 2
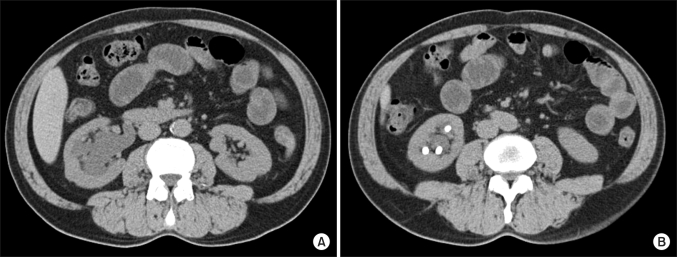
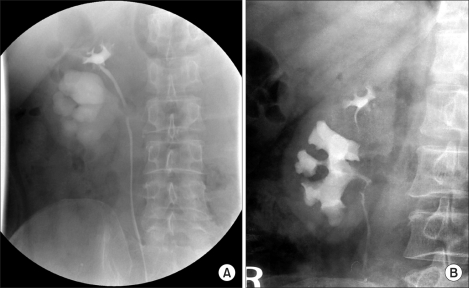
A 54-year-old man was referred to our institution for investigation of persistent pyuria. The abdominal computerized tomography demonstrated an incompletely duplicated collecting system on the right side with marked hydronephrosis and multiple renal stones of the lower pole moiety (Fig. 3). Retrograde pyelography confirmed the findings and revealed that the lower pole pelvis was extremely dilated with grade III hydronephrosis, which suggested concomitant lower pole UPJO (Fig. 4A). On the basis of these findings, a right lower pole UPJO associated with multiple renal stones with an incomplete duplicated collecting system was diagnosed, and an antegrade endourologic procedure was planned.
Cystoscopy and then retrograde pyelography were performed and showed narrowing at the UPJ at the right lower moiety, with severe dilation of the adjacent lower pole of the renal pelvis. A ureteral catheter was inserted at the level beneath the UPJ of the lower pole moiety.
Next, the patient was placed in a prone position, and retrograde instillation of contrast was performed to opacify the pelvicocaliceal system. Percutaneous access was established at the mid calyx, and then tract dilation was performed by balloon dilation with a 30 Fr catheter at a pressure of 12 atm. Through the 30 Fr Amplatz sheath, the stones were fragmented by using a pneumatic lithotriptor under fluoroscopic control. All stone extractions were successful, and we found no evidence of residual calculi on imaging.
After a 21 Fr sheath was advanced up to the renal pelvis, the UPJO was identified easily. The narrowed ureter was incised with a cold knife as far as the periureteral fat and visualized widely. A 6 Fr Double J stent was placed in the lower pelvis for 4 weeks. Postoperative intravenous pyelography confirmed that the obstruction had been successfully relieved and that all renal stones had been successfully removed (Fig. 4B).
DISCUSSION
Ureteral duplication is the most common congenital urinary tract anomaly. The embryological concept proposed to explain the association of ureteral duplication with abnormal bifurcation of the ureteral bud is as follows. When the ureteral bud bifurcates shortly after its origin from the mesonephric duct, incomplete ureteral duplication occurs. If the two buds develop close to the normal points of ureteral origin, from the mesonephric duct, a complete duplication results [1].
However, ureteral duplication associated with UPJO is rare, and most cases occur in the lower pole of an incompletely duplicated system. This occurs as either a congenital or an extrinsic compression with aberrant or accessory renal vessels. In addition, high-grade vesicoureteral reflux may play a casual role in the evolution of some cases of UPJO. It is postulated that dilatation of the collecting system as the result of reflux may lead to elongation, tortuosity, kinking, and fibrosis of the ureter. This may be complicated by fixation of the UPJ from periureteral inflammation, leading to persistent UPJO [2].
It is likely that the cause of UPJO in our patients was congenital. During fetal life, the ureter undergoes a continuous process of obstruction and recanalization, which, if incomplete, may produce narrowing and obstruction [3]. In addition, Johnston reported that the fetal ureter may show intraluminal muscular invaginations or folds, which can persist postnatally, and they may produce UPJO [4].
Surgical treatment of lower pole UPJO must be planned so that as much functioning renal parenchyma as possible is spared. Dismembered pyeloplasty, end-to-side pyeloureterostomy, and ureterocalicostomy all are potential surgical treatments; these options should be tailored and modified depending on the intraoperative findings at the time of the procedure [5]. According to Shelfo et al, an ipsilateral pyeloureterostomy (IPU) is a common surgical procedure used to manage ureteral duplication with lower pole UPJO [2]. Open IPU has achieved success rates of 90%. However, open pyeloplasty has several drawbacks, including substantial postoperative pain due to the flank incision and prolonged convalescence. To minimize morbidity, several endoscopic techniques have been developed as alternatives to open surgery, and the endoscopic approach to UPJ has been successful for both the anterograde and retrograde procedures, offering the advantages of shorter operative time, less morbidity, reduction of postoperative analgesic requirements, and shorter hospital stay [6].
The minimally invasive techniques that have been developed over the recent past continue to evolve. Since Chandhoke et al described the Acucise® endopyelotomy in 1993 [7], it has been used for dramatic advances in the field of endourology and has allowed for precise, directed endopyelotomy procedures to be performed with high immediate success rates of 87.5% to 100%, the variance of which most likely reflects patient selection [8]. Long-term patency, however, is reportedly 61.5% to 85% after 37 to 60 months of follow-up [9]. The time to failure after endopyelotomy averages 10 to 20 months, but it is becoming increasingly clear that patients treated with endopyelotomy require longer follow-up with renal scintigraphy or intravenous pyelography. Doo et al reported that the failure rate after endopyelotomy does not nadir until 36 months [6].
The main conditions that decrease the success rates of antegrade or retrograde endopyelotomy are the presence of crossing vessel adjacent UPJO, a very large renal pelvis, and a high insertion of the ureter into the renal pelvis [6]. Additional contraindications include extensive periureteral fibrosis, a bleeding diathesis, a ureter too small to accommodate an endopyelotomy stent, and a long, (>2 cm) stenosed ureteropelvic segment. But, even in these cases of endourologic failure, salvage pyeloplasty can provide long-term patency, especially if the failure is due to an initially missed crossing vessel or a redundant renal pelvis. Braga et al reported a 100% success rate after salvage pyeloplasty over an average follow-up of 47 months [10].
Although open pyeloplasty remains the standard treatment, the minimally invasive endoscopic procedures are an attractive option and could be the first line of treatment if proper patient selection is used, for example, for UPJO resulting from an aperistaltic segment or minor stricture in the absence of a crossing vessel. With respect to long-term outcomes, these endourologic procedures may be limited, but endourologic failures can be salvaged with pyeloplasty in most cases.

 XML Download
XML Download