

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Angiomyofibroblastoma is a rare tumor that occurs in the genital tract, vulva, perineum, and pelvis of women. In men, angiomyofibroblastoma-like tumors are known to occur in areas such as the inguinal area, scrotum, and perineum. In 1997, Nucci et al first described an angiomyofibroblastoma-like tumor as a cellular angiofibroma [1]. Thereafter, in 1998, Laskin et al termed it an angiomyofibroblastoma-like tumor [2]. Clinically, the tumor has asymptomatic, well-circumscribed, and slowly growing characteristics. We experienced a case of an angiomyofibroblastoma-like tumor in the scrotum that was the first in Korea. Here, we report our case with a review of the literature.
CASE REPORT
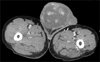
A 71-year-old man visited us with a chief complaint of a 1-year history of a mass in the right scrotum. The patient had a 15-year-history of stroke and hypertension, for which he was receiving medical treatment. The patient also had an 8-year-history of hypertensive end-stage renal disease, for which he was receiving hemodialysis three times a week. On the physical examination at the time of admission, a hard, painless mass was palpated in the right scrotum that could not be differentiated from the testis. On hematology, tumor markers such as alpha-fetoprotein, beta-human chorionic gonadotropin, and lactate dehydrogenase were all found to be normal. Scrotal ultrasonography showed a giant mass of 12 cm in size in the right scrotum. No abnormal findings were found in the bilateral testes. Abdominal computed tomography scans showed a solid, contrast-enhanced mass in the right scrotum. No findings were suggestive of lymphadenopathy or distant metastasis (Fig. 1). We suspected that a tumor had developed in the scrotum and made an incision in the right scrotum with the patient under spinal anesthesia. We identified a tumor that was definitely separated from the right testicle and excised it. The removed tumor was 13×10×6 cm in size and had an oval shape; it was encapsulated and its cross-section was composed of white mucoid components. The sporadic presence of a solid part was confirmed, but there was no concurrent necrosis or bleeding inside. Small and medium-sized blood vessels were shown under light microscopy. In the adjacent area, spindle-shaped cells were arbitrarily arranged or surrounded the blood vessels obscurely. There were no infiltrative findings to the adjacent area (Fig. 2). Immunohistochemical staining showed negative findings for desmin, S-100, and CD34. We diagnosed an angiomyofibroblastoma-like tumor that had occurred in the scrotum. Two months postoperatively, the patient is currently being followed up in an outpatient setting and has had no local recurrence.
DISCUSSION
Embryologically, various tissues such as the epithelium, mesothelium, and other tissues are derived from the mesoderm in the scrotum. For this reason, tumors occurring in the scrotum are very diverse. These tumors have different biological characteristics, for which a differential diagnosis between benign and malignant tumors and an accurate diagnosis cannot be easily made.
Of the tumors occurring in the scrotum, angiomyofibroblastoma-like tumors are a benign mesenchymal tumor with a very low incidence. Such a tumor was first mentioned by Laskin et al in 1998 [2]. Angiomyofibroblastoma was first described by Fletcher et al in 1992, which is a tumor that occurs rarely in the reproductive system of middle-aged women [3]. It particularly occurs in the vulva, labium major, vagina, areas around the clitoris, and perineal region. Despite a lower rate of local recurrence, it has histopathological characteristics that are similar to those of cellular angiofibroma and infiltrative angiomyxoma. This often leads to a misdiagnosis [3-5]. Histopathologically, there is a mixed presence of hypocellular or multi-cellular regions and the cellular morphology is diverse. Besides, there is also a mixed presence of spindle-shaped cells, satellite cells, epithelioid cells, and locally polygonal cells. These cells are arranged around the blood vessels or epithelioid-shaped regions and are accompanied by the clear presence of myofibroblastic differentiation [2,3,6,7]. Eight cases have been reported in the vulva of female patients in Korea. To date, however, no cases have been reported in male patients. Compared with the angiomyofibroblastoma-like tumors that occur in women, those occurring in male patients are seen in elderly people and have immunohistochemical differences [2]. Histopathologically, the cellular matrix of an angiomyofibroblastoma-like tumor is more dense and is abundant with collagen. Immunohistochemically, in more than half of the reported cases, tumor cells are positive for CD34 and are various for desmin. However, they are negative for S-100 protein [2]. In the present case, no immunoreactivity for CD34, desmin, or S-100 was found.
Because of the presence of histopathological characteristics that are similar to those of angiomyofibroblastomalike tumors, a differential diagnosis of infiltrative angiomyxoma cannot be easily made. It is also a benign tumor but can recur after local infiltration or surgery. An accurate diagnosis is therefore mandatory [8]. To date, only a small number of cases of angiomyofibroma and infiltrative angiomyxoma have been reported. There are no definite criteria for treatment or prognosis. It is assumed, however, that local surgical removal will be sufficient for a complete recovery.
Angiomyofibroblastoma-like tumors occurring in male patients have not been reported in Korea until now, and their incidence is extremely low. Despite the presence of benign findings on histopathology, in cases in which such tumors occur in the scrotum, both a surgical removal and a histopathologic examination are mandatory for a differential diagnosis. Furthermore, in cases of infiltrative angiomyxoma, for which the histopathologic findings are similar, a meticulous monitoring of local recurrence is essential. An accurate differential diagnosis is therefore mandatory. An appropriate follow-up observation of the long-term clinical course after the surgery is also essential.

 XML Download
XML Download