

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Because calcifications in intrascrotal organs are considered to be benign and clinically insignificant except for intratesticular calcifications, they are only briefly mentioned in urology articles and textbooks. The differential diagnosis of scrotal calcification may include calcified testicular tumors, testicular (micro-)calcification (microlithiasis), epididymal calcification, calcification of the tunica vaginalis testis, calcification of serous papillary adenocarcinoma of the tunica vaginalis, scrotal calculus (attached to the tunica vaginalis or free, including hydrocele calculus, hydrocele stone, and calculus in hydrocele fluid), and dystrophic calcification.
CASE REPORTS
During a period of 25 years, the first author operated on 42 patients with hydroceles. All of these patients were prospectively screened for calculous material in the tunica vaginalis testis.
Two patients were found to have scrotal calculi (calculi in the hydrocele fluid), accounting for an incidence rate of 4.8%. Analyses of the hydrocele stones were performed with infrared spectroscopy (Fourier Transform (FT)-IR spectrometer Spectrum BX, Fa. Perkin Elmer, Germany) based on the Atlas of Infrared Spectra for the Analysis of Concrements [1].
Case report 1
A 20-year-old white male with a small hydrocele and a palpable mass suspicious of testicular cancer on the right side underwent inguinal exploration. Frozen section pathology showed only old scars on the tunica albuginea testis. In the 10 cc clear, amber, nonmalodorous hydrocele fluid, a 2 g rough, white stone was found (Fig. 1A) that was not attached to the tunica vaginalis testis. Infrared spectroscopy revealed 100% carbonate apatite (Fig. 1B). A histological examination of the hydrocele wall was not accomplished. There were no known abnormalities in calcium, phosphorus, or parathormone metabolism. Postoperative follow-up was uneventful (Fig. 1).
Case report 2
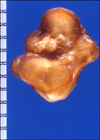
An 80-year-old patient was operated on for an asymptomatic right hydrocele. In the 300 cc clear, amber, non-malodorous hydrocele fluid between the tunica vaginalis testis visceralis and parietalis, an 11 g bizarre-shaped, brown stone without attachment to the tunica vaginalis was found (Fig. 2). Infrared spectroscopy revealed 100% carbonate apatite. A histological examination of the hydrocele wall was not accomplished. There were no known abnormalities in calcium, phosphorus, or parathormone metabolism. Postoperative follow-up was uneventful (Fig. 2).
DISCUSSION
Single or multiple scrotal calculi (hydrocele calculi, hydrocele stones, or calculi in hydrocele fluid) are freely moving concretions that lie in the space between the tunicae lining the scrotum and the testicles. They are much more common in clinical practice than what the literature would suggest, because most surgeons do not report them. Often, they are not even turned in to pathology and therefore are not described in the reports.
These calcifications are believed to originate either as fibrinous deposits in the tunica vaginalis testis after trauma or inflammation, as desquamated endothelial cells, or as remnants of the appendix testis or appendix epididymidis that have undergone torsion and become freely movable [2-4]. Hussein et al mention parasites, especially filarial worms, as one of the causes of calculi in hydroceles [5]. These organisms can be found in tropical and subtropical areas. Rare cases involve tourists. Frauscher et al found an incidence of scrotal calculi of 81% in extreme mountain bikers in addition to epididymal calcifications in 40% and testicular calcifications in 32% compared with 0% in a control group [6].
Sánchez Merino et al found 3 calculi in 2 patients with hydrocele that were white and smooth, but turned yellow and rough after removal [7]. Scanning electron microscopy and x-ray dispersion studies showed a center comprised of hydroxyapatite and white organic matter and an exterior of yellow organic matter in all 3 stones. The mineral portion of the center of the 6 mm calculus and one of the 2 mm calculi was composed of 33% phosphorus and 67% calcium; the other 2 mm calculus contained 32% phosphorus and 68% calcium by x-ray dispersion analysis. That matches well with the 100% carbonate apatite [Ca10(PO4,CO3)6(OH,CO3)2] in our patients' hydrocele stones found by infrared spectroscopy [1]. To our knowledge, this method was used for this purpose for the first time in this study. Carbonate apatite can precipitate in an alkaline milieu. During infection, extreme mountain biking and other trauma or torsion of the appendix testis, respectively, epididymis bleeding or necrosis leads to the deposit of organic matter. In the presence of high oversaturation of calcium phosphates and the absence of crystallization inhibitors in an alkaline milieu, calcification initiates and the subsequent collection of organic matter makes the process irreversible [7].
A scrotal calculus was first described during surgery in 1934 as a "fibrinoid loose body" or "scrotal pearl" (cited by [4]). Since Chatterjee (1975), about 104 cases of scrotal calculi have been reported [2,6,7,8].
Whereas 4.7% of all scrotal tissues contain calcifications, this rate is 1% for tunica vaginalis calcifications; 1.9% for calcified testicular tumors, orchitis, or testicular trauma; and 2.8% to 4.3% for scrotal calculi [8,9]. The 4.3% reported by Namjoshi at first sight matches perfectly with our rate of 4.8% [8]. But Namjoshi reported retrospectively on about 350 scrotal sonograms for scrotal swelling or pain, primary infertility, or past exposure to sexually transmitted diseases, whereas our series was prospective and only one case was operated on for symptomatic hydrocele [8]. If one looks at Namjoshi's rate of 19% (15/78) for scrotal calculi in hydroceles, the detection rate for scrotal calculi by ultrasound seems to be four times that found during operation. But these data cannot be compared because of the differences in the patient populations. Namjoshi's patients all came from subtropical and tropical areas with low hygiene standards and the possibility of parasitic infection of the scrotum, whereas the possibility for such infections was very low in our patients.
Although calculous material within the tunica vaginalis testis is considered insignificant by most authors, Sugishita et al reported on a calcified serous papillary adenocarcinoma of the tunica vaginalis [10]. Therefore, the finding of calculous or fibrous material on scrotal sonography in the tunica vaginalis testis should lead to repetition of scrotal sonography with different positioning of the patients' body (i.e., supine and lateral positions).
During sonography, calculi in hydroceles can be seen moving in the fluid between the tunica vaginalis layers; this distinguishes them from other scrotal calcifications or pathologic findings [8]. Therefore, a differentiation between a tumor and a free calculus can be made in many cases. If the calculous or fibrous material is attached to the tunica vaginalis, however, a clear differentiation between calcification and a calcified tumour may not be possible. In symptomatic cases with doubtful or suspicious sonography, an inguinal approach to surgery should be used. For asymptomatic patients, a close follow-up including palpation and sonography is recommended. Infrared spectroscopy reveals the mineralogy of the scrotal calculi after operation, which in both our cases was 100% carbonate apatite. This indicates precipitation of calcium in an alkaline milieu with infection or after trauma with bleeding like in our case 1 with scarring of the tunica albuginea.

 XML Download
XML Download