

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Fungal infections of the upper urinary tract are relatively uncommon, and fungal bezoar formation is particularly unusual [1]. Recently, I experienced an isolated pelviureteral aspergilloma in a 72-year-old woman with a solitary functional kidney. The patient presented with acute renal colic, which was initially misdiagnosed as a pelviureteral stone on nonenhanced computed tomography (CT). Here I describe this unusual case of an aspergilloma causing ureteral obstruction.
CASE REPORT
A 72-year-old woman presented to our emergency room with severe right flank pain that had developed 2 days earlier. She also complained of mild fever, nausea, vomiting, and decreased urine output. She had a nonfunctioning left kidney and a history of chronic renal failure with usual serum creatinine levels of about 2.0 mg/dl. She was neither a diabetic nor immunocompromised.
Her initial blood pressure was 130/70 mmHg and her body temperature was 37.2℃. A physical examination revealed right costovertebral angle tenderness. Initial blood tests showed leukocytosis (white blood cell count=12,700/mm3) and an elevated creatinine level (5.8 mg/dl). Her serum glucose level was 102 mg/dl. Urinalysis demonstrated hematopyuria.
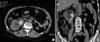
Nonenhanced CT of the abdomen revealed hydronephrosis of the right kidney and the atrophied left kidney. CT also showed a 7 cm dumbbell-shaped lesion with areas of high attenuation in the dilated right renal pelvis and upper ureter, which suggested a pelviureteral stone as the cause of the ureteral obstruction (Fig. 1). To relieve the obstruction of the single functional kidney, a right percutaneous nephrostomy catheter was inserted on an emergency basis. Antegrade pyelography demonstrated a radiolucent filling defect in the right renal pelvis and upper ureter, which was thought to be the radiolucent stone. The culture of the urine drained from the nephrostomy yielded Enterococcus faecalis.
After 2 weeks of hospitalization, the patient's serum creatinine level decreased to 2.2 mg/dl. On ureteroscopy, a movable light yellow "stone" was found in the right upper ureter. However, it was not fragmented at all with use of an EMS lithoclast and could not be removed endoscopically. For removal of the obstructive lesion presumed to be a stone, the patient underwent a right pyelotomy, and the large dumbbell-shaped "stone" was removed intact (Fig. 2A). It had a putty-like consistency and was not firm. Histopathological examination revealed clumps of fungal organisms suggestive of Aspergillus (Fig. 2B). In addition, Gram-positive cocci with calcifications were observed in the specimen. The tissue culture of the specimen yielded both Aspergillus species and Enterococcus faecalis. Postoperatively, the patient was treated with an additional antifungal agent, itraconazole. The patient had no subsequent urinary tract infections and is now well at the 20 months follow-up.
DISCUSSION
Only approximately 60 cases of fungal bezoars of the urinary tract have been reported [2,3]. The great majority have been associated with Candida species. There have been fewer than 20 cases of Aspergillus bezoars of the urinary tract [1,2]. Although almost all aspergillosis in the urinary tract has occurred in patients with predisposing conditions, such as diabetes mellitus, therapy with immunosuppressive agents or antibiotics, intravenous drug abuse, and malignancy [1-4], the patient in this case had a history of only mild chronic renal failure. Furthermore, the initial nonenhanced CT findings did not raise suspicions of a fungus ball, but rather gave the impression of a large pelviureteral stone. The urine cultures yielded only Enterococcus species. Therefore, the patient was initially misdiagnosed as having a pelviureteral stone and an associated bacterial infection.
Because of its excellence at finding urinary stones and its value for revealing other causes of abdominal pain, nonenhanced helical CT has become the imaging modality of choice for evaluating most patients with suspected renal colic [5]. However, early diagnosis of a fungus ball remains challenging. The CT findings of fungal bezoars of the urinary tract are not specific, and have rarely been described [2,6]. While in most reported cases, radiolucent filling defects could be observed on excretory or retrograde urography. It is remarkable that in the present case the fungus ball was observed as a stone-like lesion with high attenuation areas on nonenhanced CT. These findings seemed to be derived from the encrustations of the fungus ball, because the pathological examination showed calcifications with bacterial organisms as well as mycelial clumps. The development of a fungus ball accompanied by encrustation or even hard stone formation has been reported previously [7], although no information on the appearance of the fungus ball on CT was presented. It is worth noting that fungus balls with encrustations can be seen as lesions with areas of high attenuation, mimicking a urinary stone on nonenhanced CT. Of course, to diagnose fungal infections promptly, a high index of suspicion in certain clinical settings cannot be overemphasized. In addition, multiple large-volume urine cultures may be necessary to identify Aspergillus, because a single negative culture is insufficient evidence of fungal sterility [8].
Some have suggested that large fungal bezoars in the upper urinary tract can be managed safely and effectively by endourological methods [9]. In this case, however, pyelotomy was more adequate for removing the fungal bezoar completely without causing further damage to the solitary functional kidney. Fungus balls in the upper urinary tract that are not too large can be initially treated with antifungal agents before surgery [4,10]. In this case, antifungal therapy was not considered preoperatively because the patient was misdiagnosed with a urinary stone.

 XML Download
XML Download