

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Prostatic calculi are common, but most cases are asymptomatic.1 Prostatic calculi can sometimes protrude into and obstruct the prostatic urethra, although this is rare. Here we report a case of large bladder calculi with large, multiple prostatic calculi that caused urethral obstruction.
CASE REPORT
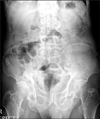
A 66-year-old man presented with significant voiding difficulty and urge incontinence. Prior treatment with an α-blocker at a local hospital failed to provide clinical improvement. In a rectal examination, the prostate was found to be firm and enlarged and the bladder was noted to be fully distended. Initial attempts at urethral catheter insertion were unsuccessful. Urethrocystoscopy revealed multiple large prostatic calculi protruding into the prostatic urethra as well as several bladder calculi. With guidewire assistance, a urethral catheter was inserted, emptying approximately 800 ml of urine. Plain abdominal radiography demonstrated multiple large prostatic calculi and 4 large bladder calculi (Fig. 1). Urinalysis revealed pyuria, and Pseudomonas aeruginosa was detected by urine culture. The prostate-specific antigen (PSA) level was within normal limits.
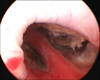
Endoscopic removal was initially attempted. Urethrocystoscopy revealed 2 large prostatic fossa just above the verumontanum containing multiple calculi of various sizes (Fig. 2). Because of the large stone burden and intraoperative hemorrhage, complete endoscopic removal was not feasible. Therefore, the decision was made to fragment the stones as much as possible and end the procedure. Postoperatively, 1 week later, the urethral catheter was removed, and several stones passed with voiding. However, urinary retention ensued. Plain radiography revealed that many fragmented calculi were located at the bulbous urethra with residual prostatic and bladder calculi (Fig. 3). Upon urethrocystoscopy, a traumatic urethral diverticulum containing several calculi at the bulbous urethra was found. Therefore, we decided to do the second operation using the open method. A low midline incision was made and the bladder was subsequently opened. Several bladder calculi remained as well as several calculi that had migrated from the prostate. After their successful removal, the posterior aspect of the bladder neck was incised and, using the surgeon's index finger, the prostatic calculi were freely dissected and extracted with long forceps. Next, urethral diverticulectomy with removal of all diverticular calculi was performed through the perineal incision. The procedure was closed after verification of the acalculus state by fluoroscopy.
The urethral catheter was removed 1 month postoperatively. The patient voided well without any urine leakage and plain radiography showed no residual calculus within the urinary tract (Fig. 4).
DISCUSSION
Prostatic calculi are exceedingly rare in children and infrequent before the age of 40 years, although they are common in males over 50 years.1,2 It is generally accepted that the formation of prostatic calculi comes with aging and typically carries no clinical significance; however, the etiology of prostatic calculi remains unclear. True prostatic calculi are formed by the deposition of calcareous material on the corpora amylacea.1 Some reports assert that many contain constituents found only in urine and not in prostatic secretions.3,4 Thus, intraprostatic urinary reflux may be implicated in the formation of prostatic calculi.5 Infection is likely another contributing factor. Prostatic calcifications are frequently identified in patients with prostatitis, but, although their presence may contribute to the chronicity of the problem (secondary to associated infection), prostatic calcifications are not believed to be the direct result of the disease itself.1
To date, there has been no consensus regarding the optimal treatment for symptomatic prostatic calculi given the lack of cases. A transurethral or suprapubic prostatectomy is generally contemplated. In the presence of multiple symptomatic calculi and intractable infection, total prostatectomy and bilateral seminal vesiculectomy, although radical, may be considered.1 Recently, there has been a trend toward endoscopic removal due to superior equipment and operating skills.6,7 Bedir et al8 reported the successful treatment of multiple prostatic calculi endoscopically. However, they approached the calculi transurethrally and suprapubically through a suprapubic incision. Kim et al9 reported the successful removal of a giant prostatic calculus with a concurrent bladder stone transurethrally. The bladder stone was removed first followed by transurethral resection of the prostate with simultaneous removal of the prostatic calculus.
In the present case, endoscopic removal was initially attempted. However, given the large stone burden and lack of adequate working space within the prostatic fossa, complete removal of all calculi was impossible. In addition, an iatrogenic urethral diverticulum occurred due to the endoscopically fragmented calculi. Thus, an open procedure, akin to an open enucleation of the prostate for symptomatic gland hyperplasia and urethral diverticulectomy, was performed. Shah et al10 reported a similar case wherein they performed an open prostatolithotomy for the management of giant prostatic calculi after endoscopic failure.
We assert that transurethral endoscopic removal may be appropriate for simple, small, symptomatic prostatic calculi. However, in the presence of multiple large prostatic and coexisting bladder calculi, the open technique may be superior.


 XML Download
XML Download