

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Silver and Russell were the first to describe a syndrome of intrauterine dwarfism recognizable at birth with craniofacial dysostosis, hemihypertrophy, disproportionately short arms, and other anomalies.1,2 Although each of the two authors described rather different findings, the composite features were later identified with the combined term Silver-Russell syndrome (SRS). It is characterized by short stature, frontal bossing, small triangular facies, sparse subcutaneous tissue, shortened and incurved 5th fingers, and in many cases, asymmetry. The diagnosis is based on distinct prenatal growth restriction and the presence of typical dysmorphic features, including short stature and limb asymmetry.3
Bilateral cryptorchidism is a rare manifestation of this syndrome, and until now has been not described in Korea. Here we report a patient presenting with a bilateral cryptorchidism. We describe our diagnosis and treatment, for the first time, by laparoscopic orchiopexy and review the literature.
CASE REPORT
A 17-month-old child transferred from the Department of Pediatrics presented with an empty scrotum. The child was born with a weight of 1,660 g (below the 3rd percentile) at 37+4 weeks, and now had a weight of 5.8 kg (below the 3rd percentile). The medical history of the child's mother was negative for infections, exposure to a teratogen, and chromosomal abnormalities. The child presented with cardiac anomalies (atrial septal defect and pulmonary artery dilation), an umbilical hernia, intrauterine growth restriction, a triangular-shaped face, scaphocephaly, late closure of the anterior fontanel, and genital anomalies (Fig. 1).
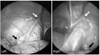
Chromosomal analysis revealed a normal 46, XY karyotype, whereas phenotypically, the external genitalia of the child included an empty scrotum without hypospadias and a micropenis. Scrotal ultrasonography detected bilateral testes in the lower abdomen; the testis sizes were 12×6×5 mm and 11×5×5 mm on the right and left, respectively (Fig. 2). Abdominal computed tomography showed no specific abnormal findings in the urogenital tract except cryptorchidism.
A laparoscopic approach was planned to perform the orchiopexy.4 A periumbilical incision was made and deepened to the rectus fascia. A 5 mm laparoscopic port was inserted under direct vision into the abdomen, and intraperitoneal insufflation was achieved with CO2 at a rate of 3 l/min. and an abdominal pressure limit of 12 mm. Bilateral testes were located 30 mm proximal to the internal inguinal ring (Fig. 3).
Laparoscopic orchiopexy was performed after placing 2 additional 5 mm ports. The dissected spermatic vessels were not enough to accomplish a tension-free orchiopexy, so we decided to perform a bilateral laparoscopic Fowler-Stephens orchiopexy.5 After creation of a new ring lateral to the bladder, both testes were situated in the scrotum. Four months after surgery, we detected no testicular atrophy, testicular retraction, or hematoma formation.
DISCUSSION
SRS is a disorder characterized by intrauterine growth restriction and typical faces. However, the clinical pattern is diverse as the result of numerous diagnostic features, reflecting a heterogeneous genetic disorder. Estimates of the incidence range from as high as 1 in 3,000 to as low as 1 in 100,000 newborns. The cause of the syndrome is still unknown, with most cases being sporadic. The early growth-restricted fetus commonly results from infection, exposure to a teratogen, or chromosomal anomalies. After excluding these etiologies, congenital anomalies can be considered. Genetically, maternal uniparental disomy of chromosome 7 is present in 7-10% of patients with SRS, and an epigenetic defect at 11p15 occurs in 60% of the patients.6
The clinical features of SRS involve poor growth, low birth weight, short height, differences in the size of the two sides of the body, and genital anomalies. These are loosely classified into major and minor features, and the more frequently observed ones are summarized in Table 1. Although no strict diagnostic criteria for SRS have been established, presence of the three major features plus one or more of the minor confirmatory features are generally required for a positive diagnosis.6 In our case, the involved diagnostic categories were intrauterine growth restriction, a triangular-shaped face, scaphocephaly, late closure of the anterior fontanelle, and cryptorchidism, but chromosomal analysis was a normal 46, XY karyotype.
The normal incidence of cryptorchidism at birth is 3%, and the incidence at 1 year is 0.8%.4 In SRS, the incidence of cryptorchidism increases to 16%. Marks and Bergeson7 described 52 males with SRS: 22 patients (42%) had unilateral or bilateral cryptorchidism, 12 (23%) had hypospadias of varying degrees, and 3 had ambiguous genitalia. Price et al8 evaluated 50 patients with SRS and reported genital abnormalities in 36%. Importantly, 13 of the 25 males required genital surgery for the condition (8 for undescended testes, 4 for hernia repair, and 1 for hypospadias). Weiss and Garnick9 reported that 42% of male patients with SRS have cryptorchidism.
In addition to the genitourinary abnormalities reported in the several cases discussed here, Haslam et al10 reported renal abnormalities (abnormal excretory urograms, unilateral chronic pyelonephritis, unilateral ureteropelvic obstruction, severe vesicoureteral reflux, and unilateral pyelonephritis). The prevalence of these abnormalities in SRS necessitates a complete urogenital evaluation, including appropriate radiologic examinations. The etiology of SRS is not clear. The genital abnormalities may be the result of reduced hormonal stimulation or resistance to hormonal influence. Further investigation into the etiology and management of this unusual syndrome will be necessary to clarify these issues.
The diagnosis of cryptorchidism in SRS does not differ from that in other conditions. So far, the treatment of intra-abdominal testes, in SRS or not, has been established. Developments in laparoscopic techniques have helped, both diagnostically and therapeutically, in the area of management of a non-palpable testis.



 XML Download
XML Download