

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Minimally invasive surgery (MIS) may already be mainstream for overall urologic surgeries. Starting from the application of endoscopy to the treatment of stones and evolving to laparoscopic surgery under pneumoperitoneum with CO2 in the 1990s, MIS is more focused than before. Now MIS faces a new challenge, "Is it possible to perform the surgery without leaving a scar?" This new task derived from a desire for the operation to be done maximally close to the meaning of 'minimal invasiveness'. Recently, several surgeons have reported a new surgical technique in which the approach is made through a natural orifice, such as the stomach, vagina, anus, or bladder, rather than the abdominal wall as in conventional laparoscopy. The new technique is modified from endoscopic and laparoscopic surgical techniques that enable both diagnosis and treatment.1-3 Here we report the first trial in Korea of a nephrectomy performed with a natural orifice approach conjoined with conventional laparoscopic techniques in an animal model. We also review the related literature.
CASE REPORT
1. Materials
Our protocol was approved by the Institutional Animal Care and Use Committee (# 08-175) in our institution, and we used a 40-kg female pig. We gained the operation field with a gastroendoscope (Lucera System®, GIF-2TQ260M, Olympus, Japan) and performed the nephrectomy with articulating laparoscopic instruments (Roticulator Endo Mini-Shears® and Endo dissector®, Tyco Health Group, USA).
2. Methods
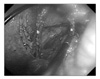
Anesthesia was induced with 5 mg/kg Zoletile and 2 mg/kg xylazine intramuscularly and enflurane endotracheally. Pneumoperitoneum was developed with CO2 gas insufflations through a Veress needle in the supine position. A gastroendoscope was introduced up to the porcine cervix, bent toward the anterior vagina wall at about a 90 degree angle, and advanced into the abdominal cavity through a 15 mm incision made with a gastroendoscopic needle knife (KD-1L-1, Olympus Medical Systems Corp., Tokyo, Japan) (Fig. 1). We confirmed the incision site and checked for bleeding from the insertion site after bending the gastroendoscope introduced into the abdominal cavity about 180 degrees. The pig was placed in the lateral decubitus position. Two additional laparoscopic trocars were inserted in the pararectal area at the level of the umbilicus, close to each other. A conventional laparoscopic nephrectomy was performed with articulating laparoscopic instruments under the gastroendoscopic vision. The margin between the intra-abdominal organ and Gerota's fascia was dissected to expose the kidney. The dissection was extended from the upper pole of the kidney to the inlet of the pelvic cavity along with the lateral margin of the colon. We displaced the colon medially. After finding the ureter within the retroperitoneal space, we dissected the posterior fascia of the retroperitoneal space, and approached the renal hilum along the dissected ureter. The proximal ureter in the renal hilar area was separated with renal vessels. The renal artery and vein were ligated with a laparoscopic clip (Ligamax®, Ethicon) (Fig. 2, 3). The nephrectomized kidney was put into a laparoscopic bag and was removed through the vagina under the guidance of the laparoscope. The total procedure time was 102 minutes. The insertion time of introduction of the gastroendoscope was 7 minutes. There were no intraoperative complications related to the procedure.
DISCUSSION
MIS has recently made up a considerable portion of urological surgery. The ultimate purpose of MIS is the resection or anatomical fixation of the target organ through a smaller incision, which can minimize the worrisome residue, pain, discomfort, and paresthesia resulting from the operative scar and complications such as an abdominal hernia related to the repair of a skin incision.4 Laparoscopic surgery with CO2 gas was developed in early the 1990s, has become popular throughout the world, and has been considered to be a representative MIS. Although the operative scars with the current laparoscopic surgery are much smaller than those with past open surgeries, complications of the operative scar such as pain, infection, and hernia may still occur in the skin incisions for trocar insertions. Thus, experimental studies have been tried recently in which the target organ is operated on without an abdominal skin incision.5-7 Natural orifice transluminal endoscopic surgery (NOTES) is a new surgical technique that can be performed with a gastroendoscope introduced through a natural orifice such as the stomach, vagina, anus, or bladder, which enables the diagnosis and treatment of intraabdominal disease by endoscopic and laparoscopic surgical techniques.1 Because NOTES does not require skin incisions, complications related to skin incisions (e.g., pain, infection, hernia, and adhesion) can be prevented. This might be a key benefit of NOTES. Postoperative adhesion may occur in up to 90% of open surgeries. The degree and range of adhesion are related to the length of the skin incision. The available data show that the incidence of postoperative adhesion in laparoscopic surgery is decreased compared with that in open surgery.8 Therefore, absence of skin incisions in NOTES may minimize the postoperative adhesion of intraabdominal organs and reduce the usage of pain medications.
Currently, however, NOTES has a long way to go, based on our experience. This procedure has some issues in our experiences as well as in other reports.5 The first issue is where the perforation should be made to approach the abdominal organs. At present, experimental approaches have included the stomach, anus, bladder, and vagina in various reports.3 However, it is still difficult to conclude which approach is best without any comparative studies. In our experience, we needed time to adapt to a new orientation of the stomach approach in previous animal experiments because of the reverse vision compared with conventional laparoscopic operations. Thus, we chose a vaginal approach and could easily obtain and adapt an operation angle similar to that of conventional laparoscopic nephrectomy. Conventional laparoscopic instruments do not fit for vaginal NOTES, however, because they could not reach the target organs. Pigs weighing 35-40 kg are selected for nephrectomy and are usually considered as fully mature pigs. Therefore, we failed the first experimental trial, pure vaginal NOTES, because of the inappropriate length of the instruments inserted through the vagina. We reviewed and reproduced the literature on transvaginal hybrid NOTES, in which 1 or 2 trocars are inserted in the abdominal wall and a gastroendoscope is introduced through the vagina for operation vision.9 In our actual experiment, the first issue of obtaining a proper operation field was solved as soon as we adapted to the flexible gastroendoscopic system. Also, we noted that the application of laparoscopic instruments through the abdominal wall facilitated the dissection of the surrounding structures adjacent to the kidney and renal hilum.
This experiment has limitations in that we could not perform pure NOTES. The main issue was that appropriate instruments for NOTES were not yet available, especially to ligate major vessels. This may result in serious complications if urgent and life-threatening bleeding occurs. This should be solved for advancement of the NOTES technique in the near future. Infection through the perforated site for the gastroendoscope should be the next careful consideration.10 Because the use of a natural orifice for the approach does not guarantee an aseptic condition with usual draping, studies to reduce the chance for infection are mandatory. Furthermore, a perfect closure of the perforation site within the natural orifice is necessary. Hybrid transvaginal NOTES may be applied to nephrectomy as in the literature we reviewed, but only in women. At present, the limitations of pure NOTES, as mentioned above, have not been solved completely, and prevent us from applying this technique to a patient in the urologic field. Thus, some endourologists have suggested single minilaparotomy surgery as an alternative and have applied some of these such urologic surgeries in actual patients.
In the present study, we successfully performed a nephrectomy with hybrid NOTES in an experimental model. More urologic surgery with pure NOTES must be facilitated as soon as appropriate instruments are developed and the limitations are solved.


 XML Download
XML Download