

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Hemangiomas are rarely develop in the ureter, and it is difficult to distinguish them from malignant ureteral tumors.1-3 Most ureteral hemangiomas are diagnosed by pathologic examination after surgery. Here we describe a case of a ureteral hemangioma diagnosed by pathologic examination after endoscopic removal. We review the characteristics of ureteral hemangiomas that differ from those of malignant ureteral tumors and address the diagnosis and treatment of ureteral hemangiomas.
CASE REPORT
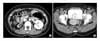
A 39-year-old woman was referred with a 1.3×1.0 cm hyperechoic mass in the posterior bladder wall detected by abdominal ultrasonography during a regular medical checkup. Her vital signs such as blood pressure, pulse rate, and body temperature were normal, and there were no abnormal findings in blood tests, urinalysis, and urine cytology. A computed tomography (CT) scan showed hypoplasia of the right kidney with a compensatory, hypertrophy of left kidney; an approximately 1.2 cm papillary enhancing lesion in the posterior bladder wall; and a soft tissue mass in the uterine cervix (Fig. 1). The soft tissue mass in the uterine cervix was proven to be clinically insignificant.
Cystoscopy showed 2 approximately 1.2×1.0 cm polypoid masses with a normal urothelial surface; the masses seemed to hang out of the right ureteral orifice to the bladder. We regarded these masses as a tumor in the bladder or ureterovesical junction, and they were electroresected by bipolar transurethral resectoscopy. Ureteroscopy identified the attachment of the tumor to the ureteral wall about 4 cm above the right ureteral orifice; however, it was impossible to advance the ureteroscope to the proximal ureter. Pathologic examination showed a ureteral hemangioma of the right ureter (Fig. 2).
DISCUSSION
Most ureteral tumors are diagnosed as malignant tumors, and benign ureteral tumors are less frequent. Among the benign ureteral tumors, the most common type is fibromyoma; hemangiomas are unusual and are rarely described in literature. Hemangiomas are the most common tumor of vascular origin, however, and result from embryological remains of unipotent angioblastic cells that develop in an anomalous way inside the blood vessels. Histologically, the lesion consists of lacunas, covered with endothelium, containing erythrocytes and organized thrombi. According to previous reports, renal hemangiomas are the most common and the next frequent urinary hemangioma is hemangioma of the bladder.1 Hemangiomas of the renal pelvis, adrenal gland, scrotum, penis, prepuce, spermatic cord, kidney, and bladder have been reported in Korea.4-7 Ureteral hemangiomas are a very rare benign ureteral tumor, and only 8 cases have been reported in the world; the ureteral hemangioma reported here is the first case reported in Korea.1-3
Clinically, patients usually presented with hematuria due to thrombus, infarction, and angiogenesis by erosion of the urothelium. Flank pain due to ureteral obstruction was reported, although some patients may be asymptomatic.1,2 These signs and symptoms are nonspecific, and patients with ureteral malignant tumors, ureteral stones, and retroperitoneal diseases may have the same symptoms.
Radiologic studies such as intravenous pyelography and CT scans are necessary tests for diagnosis; however, ureteral hemangiomas are usually noted as an uncharacteristic ureteral filling defect in these tests. Therefore, intravenous pyelography and CT scans are not helpful diagnostic tools for distinguishing ureteral hemangiomas from other ureteral tumors. In this circumstance, ureteroscopy is considered to be a useful diagnostic test.4,5,8 Under ureteroscopic examination, ureteral hemangiomas appear as a polypoid mass with intact urothelium existing in the ureteral lumen or protruding to the bladder by peristaltic movement of the ureter. Urine cytology is the most important diagnostic test to rule out a malignant ureteral tumor, and the test should be performed when a ureteral tumor is suspected.5 The results of urine cytology are normal with a ureteral hemangioma.
The patient in the present case was asymptomatic and had normal urine cytology results. Ureteroscopy revealed a polypoid tumor with intact urothelium hanging out of the right ureteral orifice to the bladder. In this case, the CT scan showed hypoplasia of the right kidney, unlike the report by Biyani et al,3 who described hydronephrosis with a ureteral hemangioma of the distal ureter. In addition, it was impossible to examine the proximal ureter above the tumor because the ureteroscope could not be advanced. Therefore, we suspect that the tumor was not dragged down by ureteral peristaltic movement but was hung out of the ureter by a different cause. We assumed that the tumor had migrated to the distal ureter because the size of the tumor was increased due to the limited ureteral luminal space and obstruction of the proximal ureter.
Hemangiomas spontaneously regress as a result of fibrosclero sis and, therefore, if asymptomatic, do not need treatment in some cases.1 Previously, it was difficult to discriminate between the benign and malignant ureteral tumors; therefore, ureteral hemangiomas were treated by nephroureterectomy or distal ureterectomy with ileal substitution if the tumor was in the distal ureter.1-3,5 Ureteral hemangiomas are benign; therefore, endoscopic removal of ureteral hemangiomas is considered one of the treatment methods.2,5,6,9,10 However, it is hard to choose a treatment method because of the relatively high incidence of malignant ureteral tumors and the fact that ureteroscopy cannot discriminate between benign and malignant ureteral tumors in all cases. Thus, urine cytology is helpful for distinguishing between benign and malignant ureteral tumors. Moreover, frozen sections of the ureteral tumor prepared during surgery may help to diagnose and choose the treatment method.2 In the present case, urine cytology was normal and ureteroscopy showed a polypoid tumor with an intact urothelium. Therefore, we considered this mass to be a benign tumor and resected it endoscopically.
Ureteral hemangiomas are very rare, benign tumors that are difficult to discriminate from malignant tumors and therefore are generally diagnosed by pathologic examination after surgery. However, urine cytology, ureteroscopy, and frozen sections prepared during surgery may help to discriminate between malignant tumors and benign tumors such as hemangiomas. In conclusion, we suggest that unnecessary radical surgery can be prevented when physicians keep the possibility of a benign ureteral tumor in mind during evaluation.

 XML Download
XML Download