

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Primary signet ring cell carcinoma of the urinary bladder is an extremely rare variant of adenocarcinoma that was first described by Saphir1 in 1955. This tumor initially presents as a high-grade, high-stage lesion, because the neoplasm diffusely invades the bladder wall without forming intraluminal growth. As a result, patients have no specific symptoms, which leads to delayed diagnosis and poor prognosis.2 We present 2 cases of primary signet ring cell carcinoma of the urinary bladder with a brief review of the current literature.
CASE REPORTS
CASE 1
A 35-year-old man was admitted after experiencing painless gross hematuria for 3 months. The patient had no concomitant medical history or familial history of any malignancy. Laboratory data were within the normal ranges except for many red blood cells on urinalysis. Atypical cells were found on urine cytology. On cystoscopy, a sessile tumor was found which extended from the right bladder wall to the dome. Computed tomography showed an approximately 4 cm mass with calcifications on the right bladder wall. No lymph node enlargement or distant metastases were observed. Tissues were taken by transurethral resection. Microscopically, the mass showed a signet ring cell feature, with abundant mucin, confluent necrosis, and calcification. We performed a complete gastrointestinal endoscopic evaluation and analysis of tumor markers to exclude an extravesical primary tumor site, but no other primary site was found. The tumor was considered to be a primary signet ring cell carcinoma of the urinary bladder, and the patient underwent radical cystectomy with an ileal conduit and bilateral pelvic lymphadenectomy.
The surgically obtained urinary bladder revealed a protruding mass lesion measuring 6.0 cm in diameter from the right anterior wall to the dome. Microscopically, the tumor mass was composed of signet ring cells with an abundant mucin pool that was invading the perivesical adipose tissue. Adjacent mucosa revealed cystitis glandularis. The histopathological staging was pT3bN1M0. Postoperative adjuvant chemotherapy was not performed because the patient refused. The patient was free of local recurrence or distant metastasis until 28 months after the operation. At 34 months postoperatively, the patient presented with back pain, nausea, vomiting, and constipation. Multiple metastases to the ribs, spine, and pelvis were noted on whole-body bone scan and metastatic nodules in the liver were also noted on computed tomography. The patient went on to receive radiotherapy (3,000 cGy every 3 weeks) and received adjuvant chemotherapy with the M-VAC regimen (methotrexate, vinblastine, adriamycin, and cisplastin). The patient died at 37 months postoperatively.
CASE 2
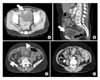
A 57-year-old woman was referred to our hospital for a recent episode of painless total gross hematuria. The patient presented with complaints of voiding symptoms such as frequency and urgency. The patient denied any medical history or family history, and laboratory data were within normal limits except for microscopic hematuria on urinalysis. A whitish, sessile mass that extended from the anterior bladder wall to the dome was noted on cystoscopy. On computed tomography, an invasive bladder tumor that extended to the anterior omentum and mesenteric fat was seen (Fig. 1). Tissues were taken by transurethral resection. Microscopically, the resected fragments of the mass were almost entirely tumor cells showing signet ring cell features with abundant mucin. There were also some fragments of surface urothelium showing intestinal metaplasia (Fig. 2). Primary tumoral site work-up was done with [18F] fluorodeoxyglucose-positron emission tomography (FDG-PET), gastrointestinal endoscopic examination, and tumor marker analysis. The FDG-PET revealed a metastatic focus at the omentum (Fig. 3). No other primary site was found. The serum levels of carcinoembryonic antigen (CEA) and cancer antigen 125 (CA 125) were 1.95 ng/ml (normal, <5 ng/ml) and 65.77 U/ml (normal, <35 U/ml), respectively. In addition, gynecological evaluation also revealed no specific findings. Primary signet ring cell carcinoma of the urinary bladder was considered, and the patient underwent partial cystectomy and planned adjuvant chemotherapy. In the surgical field, we grossly identified peritoneal carcinomatosis.
The partially resected urinary bladder revealed a 3.5 cm solid mass lesion with a mucoid cut surface. Microscopically, the tumor mass was composed of nests or lobules of signet ring cells with dissecting mucin pools. The tumor cells were infiltrating the perivesical fat tissue (pT3bN0M1). Postoperative adjuvant therapy was not done because of the patient's refusal.
DISCUSSION
Primary signet ring cell carcinoma of the urinary bladder is a relatively rare subtype of adenocarcinoma and comprises only 0.5-2% of all primary cancers of the urinary bladder.2 Since its initial description by Saphir1 in 1955, approximately 70 cases have been reported worldwide,3 and 3 have been reported in the Korean literature.4,5
Bladder adenocarcinoma may be very difficult to rule out because it has the same histologic and immunohistochemical features as urachal carcinoma. Signet ring cells can also be found in adenocarcinomas of urachal origin. Several criteria for classifying a tumor as urachal in origin have been suggested. Johnson et al proposed the following criteria6: 1) tumor in the bladder (dome), 2) a sharp demarcation between the tumor and the surface epithelium, and 3) exclusion of primary adenocarcinoma located elsewhere that spread secondarily to the bladder. The present cases showed intestinal metaplasia in surface epithelium in case 2 cystitis glandularis in case 1. There were no sharp demarcations between the tumor and the surface epithelium. Thus, we can exclude a urachal tumor in origin, although the tumors occurred in the anterior wall to dome.
The histogenesis of primary nonurachal mucin-producing adenocarcinomas including signet ring cell carcinomas remains unclear, because the normal bladder contains neither columnar nor mucus-secreting glandular epithelium. Such adenocarcinomas are considered to arise directly from the totipotent cells of the transitional epithelium,3 but stepwise development from preexisting transitional cell carcinomas by a metaplastic process is assumed to occur more frequently.7
Primary signet ring cell carcinoma of the urinary bladder generally occurs in middle age and is usually diagnosed at an advanced stage, usually demonstrating a subsequently poor prognosis.2 In our cases, both patients were initially diagnosed as having bladder cancer with perivesical invasion (T3b). The usual clinical presentation does not differ significantly from that of other bladder malignancies.2 Hematuria and irritation on voiding are the most common presenting complaints. In addition, the patient in case 1 developed the tumor in the fourth decade of life, a relatively young age compared with the conventional age of incidence of bladder cancer.
Cystoscopic findings of signet ring cell carcinoma are usually no obvious mucosal lesion. The mucosal surface is described as simply edematous, bullous, and erythematous. When a mass lesion is recognizable, it is described as pedunculated, polypoid, sessile, and ulceroinfiltrative.8 Both of our cases had a huge, sessile mass that could be detected grossly by cystoscopy.
Primary signet ring cell carcinoma of the urinary bladder has the same histology as that of the gastrointestinal tract, breast, lung, gallbladder, and prostate; therefore, further evaluations for other primary sites are mandatory to exclude metastasis. In our cases, the gastrointestinal evaluation included esophagogastroduodenoscopy and colonoscopy. But we found no other tumor lesions. Although there is no established serum marker of primary signet ring cell carcinoma of the urinary bladder, elevated CEA has often been reported. Yamamoto et al9 reported that the serum level of CEA is normalized postoperatively and gradually increases as the disease progresses. Therefore, they have suggested that CEA might be used for determining malignant potential and for monitoring signet ring cell carcinoma. In both of our cases, CEA elevation was not noted.
Treatment modalities for signet ring cell carcinomas include surgery, radiotherapy, and chemotherapy. Surgical options range from transurethral resection to radical cystectomy with urinary diversion. Most of the reported cases have undergone radical cystectomy with urinary diversion. But because most of these cancers were diagnosed at an advanced stage, the prognosis was very poor.2 In the present case 2, partial cystectomy and adjuvant chemotherapy were planned because of the peritoneal metastasis at diagnosis. Radiotherapy and chemotherapy alone have had limited success and are usually used as adjuvant therapy after surgery. Recently, Hirano et al10 reported successful treatment with intra-arterial chemotherapy alone for invasive primary signet ring cell carcinoma of the urinary bladder. However, the appropriate chemotherapy regimen and the method of injection have not yet been established.
To improve the prognosis of primary signet ring cell carcinoma of the urinary bladder, early diagnosis and establishment of the more effective chemotherapy regimen would be necessary.


 XML Download
XML Download