

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Metastatic tumors of the paratesticular tissue are rare. The common primary sites of metastasis of the paratesticular tissue are the prostate, kidney, gastrointestinal tract, lung, and breast [1,2]. Gastric cancer usually invades the regional lymph nodes, liver, lung, bone, and brain. The paratesticular tissues are rare sites of metastasis from a gastric carcinoma. Here we report the first clinical case of a metastatic tumor of the tunica vaginalis and epididymis associated with a hydrocele that originated from occult gastric cancer.
CASE REPORT
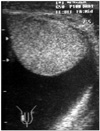
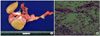
A 72-year-old patient who had been prescribed medication for benign prostatic hyperplasia showed a painless mass in the right scrotum. The mass was incidentally discovered 2 months previously and had gradually increased in size. In a physical examination, we detected a 7 cm, soft, nontender mass with transillumination in the right scrotum. The patient had neither history nor symptoms of any gastrointestinal abnormality. Scrotal ultrasound showed an anechoic cystic mass on the right testis that was displaced downward. The right testis and epididymis were normal in size without any mass (Fig. 1). Therefore, hydrocele was suspected and a scrotal incision was performed. During the operation, we found an ill-defined, grayish, localized mass-like lesion measuring about 1.3×0.8 cm in the epididymis. Frozen biopsy further revealed an atypical, round, clear cell infiltrative lesion into smooth muscle bundles, which did not exclude malignancy of the paratesticular tissue. The operation was therefore converted to a radical orchiectomy with an additional inguinal incision. The pathological diagnosis was a moderately to poorly differentiated signet ring cell-type adenocarcinoma involving the tunica vaginalis, epididymis, and surrounding soft tissue (Fig. 2). The results of immunohistochemical stains were positive for cytokeratin, carcinoembryonic antigen, and PAS. Because we suspected metastatic cancer, prostate-specific antigen measurement, colon imaging study, gastrointestinal fibroscopy, and abdominal computerized tomography were performed to detect the primary cancer. The gastrointestinal fibroscopy showed a huge mass in the antrum and biopsy revealed a signet ring cell-type adenocarcinoma. Abdominal computerized tomography uncovered a heterogeneous tumor with an irregular margin in the antrum and body of the stomach associated with multiple hepatic metastases and multiple retroperitoneal lymphadenopathies (Fig. 3). On the basis of these findings, the patient was diagnosed as having a metastatic paratesticular adenocarcinoma originating from a gastric carcinoma with retroperitoneal lymphadenopathy and hepatic metastasis. Accordingly, the patient received cisplatin-based chemotherapy but died with multiple organ failure 3 months after the operation.
DISCUSSION
Less than 50 cases of solid tumor metastasis to the epididymis, with or without spermatic cord involvement, have been reported. Many of these were incidental discoveries at autopsy or examination of orchiectomy specimens removed therapeutically for prostate cancer [3]. The prostate is the most common primary site for testis metastasis from epithelial tumors (37%). Other common primary sites are the stomach (18%), kidney (16%), colon (13%), carcinoid tumor (8%), and pancreas (5%) [4]. In Japan, a paper reported a total of 84 cases of metastatic tumors of the spermatic cord, approximately half of which were metastases from gastric cancer [5]. This may be the result of the comparatively small number of prostate cancer cases in Japan and a therapeutic modality in prostate cancer with less invasive treatments like hormonal treatment.
Several routes of metastasis to the tunica vaginalis and epididymis have been proposed, such as direct extension from adjacent organs (particularly in a prostatic carcinoma), intraductal spread via the vas deferens, retrograde venous and lymphatic extension, and arterial embolism. In our case, the route of lymphatic extension was suspected, particularly in view of the multiple retroperitoneal lymphadenopathies.
Ultrasonography, the imaging modality of choice, may help in the diagnosis of a secondary tumor, especially in the presence of nodules and a recent diagnosis of another primary cancer [6]. In the present case, the patient had neither symptoms nor history of gastrointestinal tumors with any abnormality except hydrocele in sonography. Hence, it was difficult to find the tumor without operating.
The treatment modality for a primary malignant tumor of the epididymis and a secondary tumor does not differ because chemotherapy is the only possible option at this distant metastatic stage. The prognosis of this cancer was unfavorable, because metastatic tumors to the paratesticular tissues are usually identified in the setting of disseminated disease. As shown in our case, the results were disappointing.
It is very rare for a paratesticular metastasis to present as the first manifestation of an occult primary neoplasm. We found only one reported case of a metastatic tumor to the spermatic cord that originated from occult gastric cancer [7]. In most cases, the patients had a history of gastric cancer [5,8,9]. Our report may be the first case of scrotal hydrocele as the first manifestation of occult gastric cancer that metastasized to the tunica vaginalis and epididymis.

 XML Download
XML Download