

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Testicular cancer is the most common urological cancer among young men. The incidence of testicular cancer has increased steadily since the last century. But cancer of pexed testis is relevantly rare disease. We report a case of testicular cancer of 24-year old men who received orchidopexy at age of 8 years.
CASE REPORT
A 24-year-old man who had right orchidopexy at age of 8 years presented with right testicular pain for 3 weeks. On physical examination, both testes were located in scrotum and a nodular tender mass was palpated in right epididymal area. Epididymitis was suspected and the patient received antibiotic medication.
Ultrasonography showed 2 cm sized round shaped hypoechoic mass with focal areas of increased echogenicity in right testis. The mass showed focal bulging contour which suggestive of tunica albugineal invasion (Fig. 1). Alpha-fetoprotein and beta-human chorionic gonadotropin were 3.13 ng/ml and 0.928 mIU/ml, respectively.
Right testis was explored through inguinal approach and found to have a hard irregular mass on upper pole area. The testis was removed with high ligation of spermatic vessels.
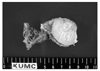
Cut surface of the specimen showed an ill-demarcated, pale tan to white and solid mass, measuring 1.2×1.0×1.2 cm in size (Fig. 2).
On microscopic examination, the mass consisted of solid sheets or glandular pattern of undifferentiated cells with marked coagulative necrosis. There were typical, large, irregular and vesicular nuclei with prominent macronucleoli. There was no evidence of other germ tumor components in this specimen. Immunohistochemistry revealed diffuse strong cytoplasmic staining for cytokeratin and membranous staining for Ki-1 (CD30) (Fig. 3). These microscopic and immunohistochemical findings were identical to the embryonal carcinoma. Tunica albuginea was involved by scattered clusters of tumor cells and foci of vascular invasions. There were scattered foci of vascular invasion in epididymis (Fig. 4). Spermatic cord was not involved by tumor.
An abdominal computed tomography showed no evidence of tumor metastasis.
This patient still alive in good heath for 2 years after operation.
DISCUSSION
Undescended testis is associated with a 3-10-fold increase in the risk of testicular cancer than normal testis.1 Approximately 10% of testicular cancers arise from an undescended testis, and 7 to 10% of patients with testicular cancer have a prior history of cryptorchidism.2,3
The association between cryptorchidism and testicular cancer might be explained by 2 theories; the common cause theory which related to a common hereditary or environmental factor and the position theory that an abnormal location of testis in suboptimal microenvironment and macroenvironment to develop cancer.4 There are disputes on reducing the increased cancer risk of orchidopexy. Prener et al5 reported that there was no decrease in the risk for testicular cancer associated with undescended testis after correction in early childhood. Pike et al6 reported that there was no correlation between the age at orchidopexy and the risk of subsequent malignancy. But orchidopexy had benefit because the resultant scrotal position is optimal for the early detection of malignant change.7
Recently, Walsh et al8 reported a beneficial effect of early orchidopexy for testicular cancer with systematic review and meta-analysis of the literature. They concluded that prepubertal (before age 10 to 11 years) orchidopexy may decrease the risk of testicular cancer, thus early surgical intervention is indicated in children with cryptorchidism.
The most common tumor that develops from a undescended testis is seminoma. But in pexed testis nonseminomatous tumors are predominant. Jones et al9 reported 34 cases of testicular cancers associated with undescended testis. Nonseminomatous tumors were predominant in patients who had prior orchidopexy (78%, 7/9), and seminomas were predominant in patients with uncorrected undescended testis (64%, 16/25). The number of cases which stages III and IV are 4 (44%) in prior orchidopexy group and 4 (16%) in uncorrected group. Because the higher proportion of advanced nonseminomas in prior orchidopexy group, 4 (44%) in prior orchidopexy group and 6 (24%) in uncorrected group were died. The relationship between early orchidopexy and more favourable disease stage is not statistically significant. And the age at orchidopexy and pathological type had no correlation.
In this case, our patient received orchidopexy at age of 8 years, and showed embryonal carcinoma with favourable stage. He is still in good health, but intensive follow up may be needed.



 XML Download
XML Download