

 PDF
PDF ePub
ePub Citation
Citation Print
Print


PURPOSE
To aid in the induction of pregnancy for males with obstructive azoospermia or sperm excretion disorders, sperm can be obtained by microepididymal sperm aspiration (MESA), percutaneous epididymal sperm aspiration (PESA), testicular sperm extraction (TESE), or by electric ejaculation. However, these methods do not yield a satisfactory sperm retrieval rate or pregnancy rate. Therefore, we reported a relatively simple, newly developed method based on animal experiments that allows for the effective retrieval of a large amount of active sperm from in vitro retrieval of epididymal sperm.1 Since 1995, sperm retrieved by this procedure have been used to induce pregnancy by conventional in vitro fertilization (IVF) and intracytoplasmic sperm injection (ICSI) through either zygote intrafallopian transfer (ZIFT) or intrauterine transfer (ET). To date, a total of 62 cases have attempted this procedure. The sperm retrieval rate, fertilization success rate, and success rate of pregnancy and birth rates by this method were thus compared with the results of conventional sperm retrieval methods. In addition, the distribution of sperm within the epididymis was assessed.
MATERIALS AND METHODS
1. Patients
From September 1995 to December 2006, 51 patients with obstructive azoospermia and 11 with either a spinal cord injury or an ejaculation disorder, such as retrograde ejaculation, had sperm retrieved from the epididymis by the in vitro retrieval method. With the retrieved sperm, either IVF or ICSI was performed and 131 cycles of ZIFT or ET were subsequently performed. For all patients, a semen analysis was performed and serum luteinizing hormone (LH), follicle-stimulating hormone (FSH), prolactin and testosterone levels were measured. In addition, a transrectal prostatic ultrasonography was performed to assess the presence or absence of ejaculatory duct obstruction. A testicular biopsy was performed in cases of suspicious testicular azoospermia. Cases confirmed to be testicular azoospermia and cases with an operable obstructive azoospermia were excluded from the study. The patients with ejaculation disorders due to spinal cord injury or retrograde ejaculation were the same subjects who had a record of previous failed attempts at pregnancy by conventional sperm retrieval methods, such as electric stimulation.2 The average age of the patients was 36 years (range: 23-53 years) and the average age of their spouses was 32 years (range: 23-44 years). Results of hormonal assay were normal in all patients. The cases of obstructive azoospermia included failure of the vasal reversal after vasectomy, congenital absence of the vas deferens, epididymitis, etc. (Table 1).
2. Controlled ovarian hyperstimulation and oocyte aspiration
Controlled ovarian hyperstimulation was performed with a combination of GnRH agonist (Superfact; Hoechst, Frankfurt Germany) and FSH. The female partners received 0.5 cc GnRHa/day, seven to ten days before menstruation, and the doses were continued until the day of the hCG injection. On the third day of the menstrual cycle, FSH injection was initiated after the vaginal ultrasonogram had been reviewed. When two or more follicles were greater than 18 mm in mean diameter, 10,000 IU of hCG was given intramuscularly. Thirty-six hours later, oocytes were obtained, washed with Dulbecco's Phosphate-buffered solution (Gibco) with 40 IU/ml of heparin, transferred into Basal XI (Sage BioPharm) with 10% human cord serum (HCS) and then incubated at 37℃ in a 5% CO2 incubator (BB6220, Heraeus, Germany).
3. In vitro retrieval of epididymal sperm and sperm preparation
Just after aspiration of oocytes from the female partner, an epididymis of the corresponding patient was detached and sent to the laboratory, where we have been performing sperm retrieval with this technique since 1995.1 Favorable dishes with many motile spermatozoa were selected under the inverted microscope and suspensions of these selected dishes were combined into one or more conical tubes (12×75 mm). The collected suspension was prepared for IVF, ICSI, and cryopreservation, which we described in a previous publication.1
4. Conventional IVF and IVF with ICSI (Fertilization method)
After sperm preparation, conventional IVF was performed in Basal XI with 10% HCS when an adequate number of motile sperm was obtained (motility >25%, >20×106 motile sperm). If the number of motile sperm was not adequate for conventional IVF, ICSI was done with a micromanipulator (5171, Eppendorf, Germany) under an inverted microscope (Leitz, Germany). The ICSI procedure was performed as described previously by Palermo et al.3 After the ICSI procedure, the oocyte was transferred into Basal XI with 10% HCS and incubated at 37℃ in a 5% CO2 incubator.
5. Fertilization confirmation and embryo transfer
Sixteen to eighteen hours after the insemination or the ICSI procedure, the oocytes were examined for fertilization. Resulting zygotes from the insemination by conventional IVF were placed into transfer medium (Basal XI with 15% HCS) and a maximum of two zygotes were transferred into each fallopian tube by minilaparotomy. Resulting zygotes from the ICSI procedure were transferred into culture medium (Basal XI with 15% HCS) and incubated for an additional 72 hours and then the morphologically best embryos (up to three) were selected and transferred into the uterine cavity. The remaining sperms and embryos were cryopreserved. Progesterone administration (50-75 mg I.m/day) was started on the day of aspiration for luteal support. Fourteen days after the embryo transfer, the serum B-hCG levels were checked. Clinical pregnancy was defined as the presence of a gestational sac with a fetal heart beat during a vaginal ultrasound examination.
The statistical significance of our results was analyzed by PC-SPSS version 13.0. Depending on the cause of post-testicular infertility, patients were classified as either obstructive azoopermia or ejaculation disorder patients, and Student's t-test were applied to analyze the pregnancy success rate relative to the cause of azoospermia. Statistic significance was considered p value<0.05.
RESULTS
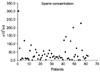
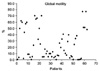
The in vitro sperm retrieval rate from the epididymis was 96.8% (60/62). For the retrieved sperm, the mean sperm concentration was 43.0×106/ml (Fig. 1), the mean volume of the final sperm suspension was 0.93 ml, and the mean sperm motility was 25.0% (Fig. 2). An average of 7.6 tubes of cryopreserved sperm was obtained per patient (Fig. 3). Analyzing the in vitro sperm retrieval rate for different areas of the resected epididymis showed that sperm was most prevalent in the head area, resulting in 40 cases of successful retrieval (64.5%). The rate decreased for each resected section in the body and decreased even more in the tail area (Fig. 4). From the 11 patients with ejaculation disorders, the average sperm concentration was 55.5×106/ml, the mean volume of the final suspension was 1.00 ml, the percent of motile sperm was 45.0%, and an average of 7.8 tubes of cryopreserved sperm was collected. As for the 51 cases of obstructive azoospermia patients, the average sperm concentration was 40.2×106/ml, the mean volume of the final suspension was 0.91 ml, the percent of motile sperm was 21.2%, and an average of 7.6 tubes of cryopreserved sperm was collected. The patients with ejaculation disorders had better results for all the measurements, but the differences were not statistically significant (Table 2).
Among 60 patients whose epididymal sperms were retrieved, 19 patients (31.7%) underwent conventional IVF and ZIFT for induction of fertilization. 11 clinical pregnancies (57.9%) were achieved. 41 patients (68.3%) underwent ICSI with fresh epididymal sperm and intrauterine transfers which resulted in 16 clinical pregnancies (39%). The excessive embryos from both procedures were cryopreserved. 6 clinical pregnancies from cryopreserved embryo transfers were achieved. A total of 27 clinical pregnancies (45%) were achieved using IVF and/or ICSI with fresh epididymal sperm. From 63 cycles fertilized by ICSI with frozen epdidymal sperm, 27 clinical pregnancies (42.9%) were achieved. Overall, the clinical pregnancy rate per couple was 77.4% (48/60). A total of 43 women gave birth; 57 neonates were born, of which there were eight cases of twins and three cases of triplets. The miscarriage rate per cycle was 14.7% (19/129) and the percentage of ectopic pregnancies per clinical pregnancy was 5.0% (3/60) (Table 3). 1 abortion case of cryopreserved embryo transfer was observed at 6 weeks after clinical pregnancy (gestational sac was noted still 5 weeks after cryopreserved embryo transfer). The cases with obstructive azoospermia had a 41.6% (45/108) clinical pregnancy rate per cycle. By comparison, the patients with an ejaculation disorder had a 60.0% (9/15) clinical pregnancy rate per cycle but the difference in clinical pregnancy rates between these two groups was not significant (Table 3).
DISCUSSION
According to the report by Silber et al.,4 in surgically uncorrectable obstructive azoospermia patients, sperm could be retrieved by the microsurgical epididymal sperm aspiration method. Nonetheless, both the fertilization rate and pregnancy rate by conventional IVF were reported as very low with MESA. In 1992, Palermo et al.3 reported a 50% pregnancy rate (4/8) per cycle by intracytoplasmic sperm injection and subsequently, ICSI contributed greatly to the improvement of both the rates of fertilization and pregnancy.
In 1997, Cha et al.5 reported the following average pregnancy rates per cycle for the different sperm retrieval methods used with ICSI: 34.6% for MESA, 24.1% for percutaneous epididymal sperm aspiration, and 34.5% for testicular sperm extraction. In addition, Nicopoullos et al.6 reviewed various reports that performed ICSI using sperm retrieved by TESE and MESA and reported diverse outcomes for these two methods in 2004.
Regarding the in vitro epididymal sperm retrieval technique, in 1995, Kim and Han reported eight cases of pregnancy by conventional IVF.1 To date, additional 62 cases of in vitro sperm retrieval have been performed. After 1995, we began to perform conventional IVF and ICSI simultaneously to improve the rate of pregnancy. In this study, the quantity and quality of sperm retrieved and pregnancy scores were comparable to those of conventional MESA, PESA, and TESE methods. Schroeder-Printzen et al.7 reported that with the MESA method, they obtained a sperm retrieval rate of over 90% and more than the average 7.6 tubes of cryopreserved sperm. According to a recent report by Lin et al.,8 PESA can cryopreserve up to 6.5 tubes. Nevertheless, Rosenlund et al.9 reported that in 20 cycles of PESA, sperm could only be cryopreserved in 9 cycles (45%).
Therefore, the retrieval rate of sperm and the number of cryopreserved tubes varies depending on the retrieval method used and it is difficult to determine whether these classic methods of sperm retrieval are superior or inferior to our technique (Fig. 3). However, the quantity and quality of cryopreserved sperm and the overall sperm retrieval rate with both MESA and PESA methods is likely to be lower because the in vitro retrieval of epididymal sperm method can dependably retrieve all the sperm from the entire epididymis. In our study, the epididymal sperm retrieval method differed too much from MESA to directly compare the quantity and quality of the respective sperm samples. For the in vitro retrieval method, the resected epididymis was divided into three parts: the head, body, and tail. Then, depending on the epididymis size, it was divided further into smaller pieces, and the sperm were retrieved firstly using 2 ml of medium solution per divided section and secondly by repetitive puncturing and squeezing of the smaller sections. After the procedure, only the dishes of sperm with good motility were collected and this yielded a suspension volume of approximately 10??0 ml. At this stage, the density of motile sperm was approximately 10%. A final preparation of the sperm with a percoll gradient resulted in the sperm samples for which the quality and quantity are shown in Table 2.
Schroeder-Printzen et al.7 reported that the sperm density after dilution of the aspirate obtained by MESA was 40.9×106 spermatozoa/ml and the sperm density was comparable to results from our technique. The motile sperm were 24.8% in their report, which is also comparable to our result of 25.0% motility. If the motility of sperm was relatively good in our study, 19 cycles of conventional IVF were performed, and from this, 11 cases of clinical pregnancies were achieved (57.9%). This result suggests that the quality of sperm retrieved by our method may be relatively better than that from the classic retrieval methods described above. However, when we performed ICSI, the pregnancy rate was comparable to that achieved with other sperm retrieval methods. Therefore, with respect to pregnancy rate, our method is not superior to other sperm retrieval methods. However, when compared to MESA, our surgical technique is more convenient, the pregnancy rate by the conventional IVF is higher, and the quality of cryopreserved sperm is comparable.
With MESA, microsurgery is essential and postoperative complications can be problematic. PESA was designed to overcome these complications; however, tissue damage may occur due to blind puncturing during the procedure.5 In 1995, Silber et al. reported that in 12 cases in which MESA was performed, sperm could not be retrieved due to severe adhesion in the vicinity of the epididymis caused by previous scrotal surgery.10 This suggests that due to complications of repeated surgical manipulations, it is important to cryopreserve sperm during sperm retrieval from the testis and/or epididymis. One of the shortcomings of TESE is that it requires resection of the endocrine organ, the testis. It has been reported that after performing general TESE, an acute inflammatory finding in the biopsy area and thrombi were detected on ultrasound. After six months, a scar and calcification occurred in this region. In addition, a small portion of cases may experience atrophy of the testis or a complete disappearance of blood flow.11 The in vitro epididymal sperm retrieval technique does not require microsurgery, the procedure is relatively simple, economical, and any damage to the testis is avoided. In addition, with TESE, the number and motility of sperm are inferior and the amount of cryopreservation is smaller than with in vitro epididymal sperm retrieval. Although the development of ICSI facilitates pregnancy with a single normal sperm with good motility, the retrieval of a large amount of good quality sperm can drastically improve the chances of becoming pregnant. The advantage of the in vitro epididymal sperm retrieval technique should be evaluated from the view of testes preservation. A shortcoming of our method is that the resection of the epididymis may be considered excessive. Nonetheless, unlike the testis, the epididymis is not an endocrinal organ and is not essential to maintain quality of life. While MESA may be more psychologically appealing because it conserves the epididymis, patients should consider complications resulting from MESA, such as the obstruction of the epididymis.
Assessment of the distribution of sperm within the epididymis revealed that the most motile and abundant sperm were detected in the head of the epididymis. It has also been reported by investigators using MESA that the majority of epididymal sperm can be retrieved from the head area of the epididymis.12 Nevertheless, we found that, a substantial numbers of sperms are also present in the body and tail of the epididymis in many cases (Fig. 4).





 XML Download
XML Download