

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Purpose
Ileoureteral substitution could be the viable option for the cases with long defects of the ureter that cannot be repaired using intrinsic urinary tract tissues. Yet it is controversial whether anti-refluxing and tailoring vesicoileal anastomosis is necessary. We evaluated the safety and efficacy of ileoureteral substitution using refluxing, non-tailoring technique.
Materials and Methods
A total of 6 patients (8 ureters) underwent ileoureteral substitution at our institution between July 2002 and March 2006. We reviewed the follow up data including clinical evaluation, excretory urography or equivalent imaging results, serum creatinine and blood gases of the patients who underwent ileoureteral substitution using refluxing, non-tailoring technique.
Results
Mean follow up duration was 16 months (range: 1-44). Mean operation time was 332.5 minutes (range: 285-480), estimated blood loss was 366.7ml (range: 200-900), time to oral intake was 5 days (range: 3-7) and postoperative hospital stay was 12.7 days (range: 8-27). Most postoperative complications, which occurred in 3 patients (50%), were minor in nature, including mild ileus and wound dehiscence. On the last excretory urography, there was no evidence of obstruction in any patient. None of the patients experienced worsened renal function or metabolic derangements.
Conclusions
Ileoureteral substitution using refluxing, non-tailoring vesicoileal anastomosis can be used safely without renal deterioration or metabolic derangement for patients suffering with complex and difficult ureteral strictures that are not amenable to more conservative measures. Further studies are needed to determine the long-term safety and efficacy.
Figures and Tables
Fig. 1
Preoperative and postoperative intravenous urography of a patient with bilateral ureteral stricture. (A) Preoperative intravenous urography demonstrates severe bilateral hydronephrosis secondary to long obliterating stricture, (B) postoperative intravenous urography demonstrates that the contrast materials are drained into the bladder without obstruction. The ileal segment (arrow) is opacified by the contrast materials.
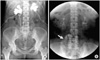
Fig. 2
Preoperative and postoperative intravenous urography of a patient with unilateral ureteral stricture. (A) preoperative intravenous urography demonstrates left hydronephrosis secondary to the ureteral stricture, (B) Postoperative intravenous urography demonstrates good drainage of contrast materials through the ileal ureter. The ileal segment (arrow) is opacified by the contrast materials.




References
1. Goodwin WE, Winter CC, Turner RD. Replacement of the ureter by small intestine: clinical application and results of the ileal ureter. J Urol. 1959. 81:406–418.
2. Mattos RM, Smith JJ 3rd. Ileal ureter. Urol Clin North Am. 1997. 24:813–825.
3. Bejany DE, Lockhart JL, Politano VA. Ileal segment for ureteral substitution or for improvement of ureteral function. J Urol. 1991. 146:302–305.
4. Gomez-Abraham I, Nguyen T, Drach GW. Ileal patch ureteroplasty for repair of ureteral strictures: clinical application and results in 4 patients. J Urol. 1994. 152:2000–2004.
5. Shokeir AA, Mahran MR, Shamaa MA. Interposition of ileum in the ureter. Scand J Urol Nephrol. 1993. 27:421–424.
6. Boxer RJ, Fritzsche P, Skinner DG, Kaufman JJ, Belt E, Smith RB, et al. Replacement of the ureter by small intestine: clinical application and results of the ileal ureter in 89 patients. J Urol. 1979. 121:728–731.
7. Monning JA, Bicknell SL. The ileal ureter in recurrent urolithiasis. J Urol. 1976. 116:699–702.
8. Shokeir AA, Ghoneim MA. Further experience with the modified ileal ureter. J Urol. 1995. 154:45–48.
9. Waldner M, Hertle L, Roth S. Ileal ureter substitution in reconstructive urological surgery: is an antireflux procedure necessary? J Urol. 1999. 162:323–326.
10. Stein JP, Freeman JA, Esrig D, Elmajian DA, Tarter TH, Skinner EC, et al. Complications of the afferent antireflux valve mechanism in the Kock ileal reservoir. J Urol. 1996. 155:1579–1584.
11. McGuire EJ, Woodside JR, Borden TA, Weiss RM. Prognostic value of urodynamic testing in myelodysplastic patients. J Urol. 1981. 126:205–209.
12. Charghi A. Ureteral replacement using a new variation of the tailored ileal segment. J Urol. 1979. 121:598–601.
13. Vatandaslar F, Reid RE, Freed SZ, Smey P, Kogan SJ, Goldsmith D, et al. Ileal segment replacement of ureter. I. Effects on kidney of refluxing vs nonrefluxing ileovesical anastomosis. Urology. 1984. 23:549–558.
 XML Download
XML Download