

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Purpose
A laparoscopic radical prostatectomy (LRP) is a less invasive alternative to a conventional radical prostatectomy. However, the learning curve for a LRP is steep; therefore, becoming skilled at the procedure is difficult. Herein, our experience of laparoscope assisted radical retropubic prostatectomy (LARRP) is reported.
Materials and Methods
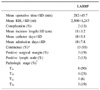
LARRP was performed on 16 patients with clinically organ confined prostate cancer. The mean age and serum prostate-specific antigen (PSA) of the patients were 63±5.7 years (51-70) and 20.01±24.8ng/ml (3.45-97.50), respectively. A longitudinal skin incision was made from the symphysis pubis to midway of the umbilicus. The incision was retracted with a self-retractor, without port placement and gas insufflation. The laparoscope was directly inserted into the wound, with modified bilateral pelvic lymph node dissection, prostatectomy and vesicourethral anastomosis performed under laparoscopic monitoring, using both open and laparoscopic instruments in the same order as for open surgery.
Results
The mean operative time was 282±45.7 minutes (200-375), including the time required for the modified bilateral pelvic lymphadenectomy. The mean estimated blood loss and specimen weight were 2,500±1,247ml (500-5,000) and 53±19.0gm (20-98), respectively. The surgical margins and lymph nodes were positive in 3 (19%) and 2 patients (13%), respectively. The mean number of dissected lymph node and incision length were 12±7.5 (4-31) and 11±3.2cm (6-15), respectively. Gradual recovery of continence occurred in 13 (93%) for 1 years after the operation.
Conclusions
LARRP is a feasible and less invasive alternative to conventional RRP, which is also devoid of the steep learning curve associated with a LRP. LARRP may be a bridge between an open RRP and a pure LRP. With the increase in the number of cases, LARRP may prove to be an effective treatment option for localized prostate cancer.
Figures and Tables


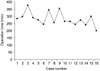 | Fig. 3Operating time of laparoscope assisted radical retropubic prostatectomy with accumulation of experience.
|
 | Fig. 4Comparison of incision length. LARRP: laparoscope assisted radical retropubic prostatectomy, ORRP: open radical retropubic prostatectomy.
|

References
1. Marshall FF, Chan D, Partin AW, Gurganus R, Hortopan SC. Minilaparotomy radical retropubic prostatectomy: technique and results. J Urol. 1998. 160:2440–2445.
2. Catalona WJ, Carvalhal GF, Mager DE, Smith DS. Potency, continence and complication rates in 1,870 consecutive radical retropubic prostatectomies. J Urol. 1999. 162:433–438.
3. Young HH. The early diagnosis and radical cure of carcinoma of the prostate. Being a study of 40 cases and presentation of a radical operation which was carried out in four cases. Bull Johns Hopkins Hosp. 1905. 16:315–321.
4. Walsh PC, Lepor H, Eggleston JC. Radical prostatectomy with preservation of sexual function: anatomical and pathological considerations. Prostate. 1983. 4:473–485.
5. Gallucci M, Vincenzoni A. Laparoscopic radical prostatectomy: a marketing or surgical strategy? Curr Opin Urol. 2001. 11:305–308.
6. Schuessler WW, Schulam PG, Clayman RV, Kavoussi LR. Laparoscopic radical prostatectomy: initial short-term experience. Urology. 1997. 50:854–857.
7. Guillonneau B, Vallancien G. Laparoscopic radical prostatectomy: the Montsouris experience. J Urol. 2000. 163:418–422.
8. Slabaugh TK Jr, Marshall FF. A comparison of minimally invasive open and laparoscopic radical retropubic prostatectomy. J Urol. 2004. 172:2545–2548.
9. Rozet F, Mongiat-Artus P, Desgrandchamps F. Hand-assisted laparoscopic nephrectomy. Curr Opin Urol. 2002. 12:229–232.
10. Lee CH, Seo SI, Kim JC, Hwang TK. Laparoscopic radical prostatectomy. Korean J Urol. 2003. 44:617–623.
11. Lee JW, Kim CS, Ahn HJ. Early and late complications of radical retropubic prostatectomy. Korean J Urol. 2000. 41:1409–1414.
12. Davidson PJ, van den Ouden D, Schroeder FH. Radical prostatectomy: prospective assessment of mortality and morbidity. Eur Urol. 1996. 29:168–173.
13. Rassweiler J, Seemann O, Schulze M, Teber D, Hatzinger M, Frede T. Laparoscopic versus open radical prostatectomy: a comparative study at a single institution. J Urol. 2003. 169:1689–1693.
14. Heinzer H, Graefen M, Noldus J, Hammerer P, Huland H. Early complication of anatomical radical retropubic prostatectomy: lessons from a single-center experience. Urol Int. 1997. 59:30–33.
15. Cho KS, Hong SJ, Chung BH. The impact of positive surgical margins on biochemical recurrence after radical retropubic prostatectomy. Korean J Urol. 2004. 45:416–422.
16. Daneshmand S, Quek ML, Stein JP, Lieskovsky G, Cai J, Pinski J, et al. Prognosis of patients with lymph node positive prostate cancer following radical prostatectomy: long-term results. J Urol. 2004. 172:2252–2255.
17. Guillonneau B, el-Fettouh H, Baumert H, Cathelineau X, Doublet JD, Fromont G, et al. Laparoscopic radical prostatectomy: oncological evaluation after 1,000 cases at Montsouris Institute. J Urol. 2003. 169:1261–1266.
 XML Download
XML Download