

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Purpose
Vascular endothelial growth factor (VEGF) is recognized as a potent constituent of the vascularization and growth of solid tumors. We assessed the serum levels of VEGF and we evaluated its correlation to the clinicopathologic findings and clinical outcome of patients with renal cell carcinoma (RCC).
Materials and Methods
Serum samples were collected before surgery from patients with RCC. The levels of serum VEGF were assessed by using quantitative enzyme immunoassay. Comparison of the serum VEGF level with the tumor stage, grade, cell type and clinical outcome was performed, and the survival rate between the RCC patients above and below the mean VEGF level was evaluated.
Results
The mean follow-up was 5.1 years. The serum VEGF level was significantly higher in the patients with RCC (mean: 497pg/ml) than that in the controls (mean: 211pg/ml) (p<0.001). The serum VEGF level was correlated with the tumor size, the pathologic T stage and the clinical stage and histologic nuclear grade, but not with the histologic subtype. Patients with a lower VEGF level (<497pg/ml) showed longer survival (p=0.0207 on univariate analysis, p=0.04 on multivariate analysis).
Figures and Tables
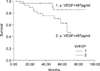 | Fig. 1Comparing the survival rate of the group with a serum vascular endothelial growth factor (s. VEGF) level>497pg/ml-renal cell carcinoma (RCC) with the group having a s. VEGF level <497pg/ml-RCC by the Kaplan-Meier curves and the log rank test (p=0.0207, log rank 5.35).
|

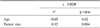
Table 2
Correlation analysis of serum VEGF with age and tumor size by Pearson's correlation coefficient analysis
![]()
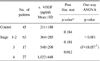
Table 3
Comparison of the serum VEGF level according to the pathologic T stage by one way ANOVA and the Post Hoc Tukey test

![]()
Table 4
Comparison of the serum VEGF level according to pathologic T stage by one way ANOVA and the Post Hoc Tukey test

![]()
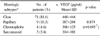
Table 5
Comparison of the serum VEGF level according to the clinical stage by one way ANOVA and the Post Hoc Tukey test
![]()

References
1. Golimbu M, Joshi P, Sperber A, Tessler A, Al-Askari S, Morales P. Renal cell carcinoma: survival and prognostic factors. Urology. 1986. 27:291–301.
2. Farber E. The multistep nature of cancer development. Cancer Res. 1984. 44:4217–4223.
3. Rini BI, Rathmell WK. Biological aspects and binding strategies of vascular endothelial growth factor in renal cell carcinoma. Clin Cancer Res. 2007. 13:741s–746s.
4. Delahunt B. Histopathologic prognostic indicators for renal cell carcinoma. Semin Diagn Pathol. 1998. 15:68–76.
5. Takahashi A, Sasaki H, Kim SJ, Tobisu K, Kakizoe T, Tsukamoto T, et al. Markedly increased amounts of messenger RNAs for vascular endothelial growth factor and placenta growth in renal cell carcinoma associated with angiogenesis. Cancer Res. 1994. 54:4233–4237.
6. Weidner N, Semple JP, Welch WR, Folkman J. Tumor angiogenesis and metastasis-correlation in invasive breast carcinoma. N Engl J Med. 1991. 324:1–8.
7. Senger DR, Van De Walter L, Brown LF, Nagy JA, Yeo KT, Yeo TK, et al. Vascular permeability factor (VPF, VEGF) in tumor biology. Cancer Metastasis Rev. 1993. 12:303–324.
8. Folkman J, Watson K, Ingber D, Hanahan D. Induction of angiogenesis during the transition from hyperplasia to neoplasia. Nature. 1989. 339:58–61.
9. Nicol D, Hii SI, Walsh M, Teh B, Thompson L, Kennett C, et al. Vascular endothelial growth factor expression is increased in renal cell carcinoma. J Urol. 1997. 157:1482–1486.
10. Fuhrman SA, Lasky LC, Limas C. Prognostic significance of morphologic parameters in renal cell carcinoma. Am J Surg Pathol. 1982. 6:655–663.
11. Zambrano NR, Lubensky IA, Merino MJ, Linehan WM, Walther MM. Histopathology and molecular genetics of renal tumors: toward unification of a classification system. J Urol. 1999. 162:1246–1258.
12. Skinner DG, Colvin RB, Vermillion CD, Pfister RC, Leadbetter WF. Diagnosis and management of renal cell carcinoma. A clinical and pathologic study 0f 309 cases. Cancer. 1971. 28:1165–1177.
13. Patard JJ, Leray E, Cindolo L, Ficarra V, Rodriguez A, De La Taillle A, et al. Multi-institutional validation of a symptom based classification for renal cell carcinoma. J Urol. 2004. 172:858–862.
14. Bouck N, Stellmach V, Hsu SC. How tumors become angiogenic. Adv Cancer Res. 1996. 69:135–174.
15. Kim JN, Song KH, Song JM. Expression of vascular endothelial growth factor and its clinical significance with neovascularization in conventional renal cell carcinoma. Korean J Urol. 2002. 43:353–359.
16. Ha HK, Ye JW, Lee SD, Chung MK. The relationship between expression of hypoxia inducible factor-1a or vascular endothelial growth factor and histopathologic characteristics in human ranal cell carninoma. Korean J Urol. 2004. 45:303–308.
17. Jacobsen J, Rasmuson T, Grankvist K, Ljungberg B. Vascular endothelial growth factor as prognostic factor in renal cell carcinoma. J Urol. 2000. 163:343–347.
18. Sato K, Tsuchiya N, Sasaki R, Shimoda N, Satoh S, Ogawa O, et al. Increased serum levels of vascular endothelial growth factor in patients with renal cell carcinoma. Jpn J Cancer Res. 1999. 90:874–879.
19. Schips L, Dalpiaz O, Lipsky K, Langner C, Rehak P, Puerstner P, et al. Serum levels of vascular endothelial growth factor (VEGF) and endostatin in renal cell carcinoma patients compared to a control group. Eur Urol. 2007. 51:168–174.
20. Zhang J, Lefkowitz RA, Ishill NM, Wang L, Moskowitz CS, Russo P, et al. Solid renal cortical tumors: differentiation with CT. Radiology. 2007. 244:494–504.
21. Douglas ML, Richardson MM, Nicol DL. Endothelin axis expression is markedly different in the two main subtypes of renal cell carcinoma. Cancer. 2004. 100:2118–2124.
22. Beecken WD, Bentas W, Glienke W, Winneweber J, Jonas D, Binder J, et al. Serum angiogenic activity: diagnostic relevance in renal cell carcinoma. Eur Urol. 2002. 42:364–369.
 XML Download
XML Download