

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Workers exposed to free silica develop nodular or stellate fibrotic lesions in the lungs that may coalesce into conglomerate or confluent lesions called progressive massive fibrosis (PMF).1) This lesion also complicate other pneumoconioses, including asbestosis, coal workers' pneumoconiosis, or mixed dust fibrosis.2, 3) PMF is inherently progressive, once started it tends to increase fairly rapidly.4) Patients with PMF are often noted to be hypoxic at rest and are prone to mycobacterial infections and spontaneous pneumothoraces and may ultimately develop fatal respiratory failure.5) However, massive hemoptysis is rarely associated with PMF. Massive hemoptysis, which is perhaps best defined as bleeding into the bronchial tree at a rate that poses a threat to life, is associated with considerable mortality unless treated aggressively.6)
We herein present an autopsy case of a silicosis patient who was complicated with PMF died with massive hemoptysis and review the reported similar cases by analyzing the papers.
Case Report
A 62-year-old man who was a stonemason for 40 years was found dead in his house to have blood in his nose and mouth. There was blood in place of the house, including living room floor, bathroom floor, and toilet. He had a history of attend to a hospital for multiple fine nodules and calcified nodules in both lungs.
At postmortem examination, there was no evidence of significant external or internal injury except few minor abrasions. There was a focus of minor subgaleal hemorrhage in a right temporal area with no bony or parenchymal injury.
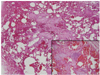
The weight of right and left lungs were respectively 722 g and 1,020 g. All lobes of the lung were hardly touched. Multiple whitish nodules which measured 0.1~0.2 cm were present in pleural surface of both lungs. Small bilateral nodules which measured more than 1.0 cm were noted in pleural surface of the upper lobes (Fig. 1). The cut surface of the nodule was whitish and solid. Emphysematous changes like honeycomb were apparent on lower lobes of the lung. Microscopically, diffuse alveolar hemorrhage was present. There was multiple patchy or nodular fibrosis with dust deposition and chronic inflammatory cells in the lung parenchyma. Some of the patchy or nodular fibrosis measured more than 1.0 cm. Small pulmonary arteries showed medial hypertrophy and fibrosis, and large pulmonary arteries showed aneurysmal dilatation (Fig. 2).
There was blood in trachea, larynx, and stomach, but not in esophagus, small intestine, and large intestine. The amount of blood was considered as a significant volume. Esophageal varix was not present. The liver revealed moderate fatty changes. Coronary arteries showed no significant atherosclerosis. The results of toxicologic study and blood-alcohol concentration were negative.
Discussion
Silicosis is a potentially fatal, irreversible, fibrotic pulmonary disease that may develop subsequent to the inhalation of large amounts of silica dust over time. In most circumstances, silicosis only develops subsequent to substantial occupational exposures.5) Free, or uncombined, silica (silicon dioxide) occurs in both crystalline and amorphous forms. Only the crystalline form, of which quartz is a major source, is fibrogenic. The pathogenesis of silicosis appears to be related to the cytotoxic action of crystalline silica on alveolar macrophages. When silica particles are not efficiently cleared from the lung by alveolar macrophages, these alveolar macrophages may become damaged. Macrophages damaged in this way are thought to become stimulated and release reactive oxygen species, reactive nitrogen species (RNS), and excess free radicals.7) When alveolar macrophages containing silica die, they release silica particles that are then re-engulfed by other alveolar macrophages, thus inducing a cycle of injury.8) The rate of disease progression appears to depend upon the rate of silica deposition in the lungs, as well as the total amount of crystalline silica that is actually retained in the lung.5)
Progressive massive fibrosis is a complication of silicosis, and may accompany other pneumoconiosis. However, it typically occurs in silicosis and coal worker's pneumoconiosis.9) It is frequently associated with functional impairment, including reduction in lung compliance, lung volume, diffuse capacity, and presence of hypoxemia.10) PMF is defined by the presence of nodular fibrosis that is greater than 1.0 cm.11) It is often characterized by large fibrotic masses in conjunction with a distortion of the lung architecture often involving an upward displacement of the mediastinal and hilar structures attributable to volume loss. In addition, lower areas of the lung may appear hyperventilated and emphysematous, often in conjunction with multiple bullae.5) Areas of emphysema cause an increased pulmonary vascular resistance due to alveolar hypoxia leading to pulmonary hypertension.12) Blood vessels around the periphery are often destroyed by the chronic inflammatory cell infiltrate and fibrosis.11)
Massive hemoptysis is a rare condition in PMF. We found several cases of massive hemoptysis in PMF complicated with silicosis. However, most of them had mycobacterial infection, which seemed to be the etiology of hemoptysis.6, 13) In this case, there was no evidence of tuberculosis, and the bleeding was originated from throughout the lungs. Accurate mechanism of massive hemoptysis in PMF, which is not combined another lung disease such as tuberculosis, bronchiectasis, or carcinoma, is not yet known. But we thought some mechanisms of that. At first, it can be arise from small friable vessels within peribronchial inflammatory tissue. Blood vessels are often destroyed by the chronic inflammatory cell infiltrate and fibrosis.11) If a great number of vessels are destroyed, massive hemoptysis can happen. The second, it can be occurred to rupture of peripheral pulmonary artery pseudoaneurysm. It is reported that a peripheral pulmonary artery pseudoaneurysm may be the source of massive hemoptysis.6) In this case, we found the large blood vessels with aneurysmal dilatations. Pulmonary artery pseudoaneurysm may develop as a result of the progressive destruction and replacement of the elastic fibers of the pulmonary artery. Partly, it can be caused by pulmonary hypertension, which is a consequence of the emphysematous area in the lung base. Finally, both can be the reason to make a massive hemoptysis.
It is known that the mortality of massive hemoptysis results from asphyxiation rather than from exsanguination.14) The deceased had blood in mouth, nose, stomach, trachea, and larynx on postmortem examination. However, these findings are nonspecific, which do not suggest the possibility of asphyxiation.
In summary, we have presented a case of the silicosis patient with a PMF, who die from massive hemoptysis. This is a rare condition, but the forensic pathologist should be aware that PMF may cause a fatal hemoptysis. There are limitations in researching the mechanism of massive hemoptysis in PMF owing to paucity of reported cases. Further study will be necessary to elucidate the relationship between the nature of PMF and the massive hemoptysis.

 XML Download
XML Download