

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
The innominate artery (the right brachiocephalic artery) is an aortic branch. From this artery, right carotid artery and subclavian artery are bifurcated. This artery is short and relatively well protected by the bony thorax.1) However, injury of this artery is not uncommon.2-4) Several cases with innominate artery injuries have been documented involving blunt traumatic injury such as motor vehicle accidents or penetrating injuries. In those cases, it isn't difficult to anticipate injuries to great vessels or determine approaches to investigate injuries, because of their trauma history, typical symptoms, and other associated injuries.
However, recently we experience a case that it appeared to be no explicit blunt trauma history, his symptoms and signs were not specific, and after the postmortem examination, the innominate arterial injury was the only isolating injury. Thus, it wouldn't have been easy to suspect this type of injury at the beginning. During autopsy procedure, looking for this injury pattern or searching for this type of injury might have also been neglected or missed. Therefore, we presented our unusual case with review of literature.
Case Report
The deceased was a 24-year-old man who went river rafting with his friends. When they had traveled nearly half of the course, they went to the riverbank to have a break and to play in the water. Some of them started diving feet first into the river near a rock so he also joined in while wearing his life vest. After diving into the water, his head was submerged for a brief moment and soon his head and body floated up. During his dive, he didn't hit anything and the water was deep enough to dive in. Nevertheless, he couldn't escape form the water and drifted down the river for about 26 meters, even though the water was not deep. Lifeguards entered the water and rescued him. After he walked out of the water, he collapsed, complaining of dyspnea and shortly thereafter, lost consciousness for a few minutes. He was transferred to a university hospital via a local clinic. There were no specific findings upon physical examination and blood tests. On radiologic examinations of the head and chest, aspiration pneumonia was suspicious. He and his family wanted to be transferred to a hospital closer to home and he left the hospital against his doctor's advice. During transfer however, he complained of dyspnea and suffered neck swelling and vomiting. He had to visit a hospital on the way, where he died. This case was reported to the police and we were consulted for the postmortem examination because the incident took place during the rafting trip and he died despite being treated in hospitals.
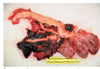
On external examination, his neck showed swelling. A small contusion was found on the anterior aspect of the right arm and the conjunctiva of his eyelids and oral mucosa were pale. On internal examination, disruption injury of the right brachiocephalic artery (the innominate artery) was found accompanied by a tearing of the blood vessel wall. The surrounding connective tissue was avulsed from the arterial wall (Figs. 1, 2). Extensive hemorrhage with hematoma was found on the subcutaneous layer and between the muscle layers on the anterior aspect of his neck. Hemopericardium (about 250 ml) and hemothorax (right about 1,700 ml, left about 700 ml) were also found with extensive hemorrhage in the mediastinum. But there were no laceration or disruption in the aortic arch or the heart. There were also no injuries on other internal organs. Toxicological study was negative except for clindamycin administrated during admission, and no diatom was found in the lung, kidney, liver, heart, or brain. The cause of death was determined as injury of the right brachiocephalic artery (the innominate artery) with extensive hemorrhage on neck and in mediastinum, both pleural cavities, and pericardium.
Discussion
Since the first traumatic avulsion of the innominate artery was reported in 1962,3) injuries of the innominate artery were not uncommon enough that some reports represented it as the second most common thoracic vascular injury after aortic disruption, or the most common aortic branch injury.1-4) Most cases were caused by neck and/or chest injuries following high energy blunt trauma or deceleration injury; motor vehicle accidents (including both restraint and unrestraint), crush injuries or falls, by penetrating injuries, and rarely by infections.1-8) In our case, we examined our case meticulously, suspicious of it being a blunt trauma, because the deceased was transferred by sudden symptoms (dyspnea, transient loss of consciousness) after diving and blunt injuries can be coupled with a drowning accident.9-10) However, we couldn't find any external and internal injuries on the chest, head and neck. Even in the police report, there was no mention of blunt trauma or penetrating injury history.
The injury mechanism is still unclear but some reports have postulated that maximum traction or shear force on the innominate artery can cause the injury,2, 3, 5-7) If blunt force was applied on the anterior wall of chest against the thoracic spine and caused compression of the chest, the heart may be displaced to the left and it lead to tension of the aortic arch. Similarly hyperextension/rotation of the neck causes traction of the right carotid artery and the shear force by longitudinal tension works on the innominate artery. Thus, either traction or shear force results in the injury of innominate artery, because the distal part of the innominate artery is mobile and aortic arch is fixed. In our case, he didn't hit any obstacles during the dive and there was no injury in his chest. So we assumed that he might have been injured during his dive from hyperextension or rotation of his neck which might be caused by the life vest related to the posture of diving feet first.
The innominate artery (the right brachiocephalic artery) is defined in three parts as follows; the proximal part indicates the vessel within 0.5 cm of the aorta, the distal part is within 0.5 cm of the bifurcation, and the middle part is in between the proximal and the distal parts.2) So the injuries of the innominate artery can be classified according to the above definitions. In most cases, the proximal part of the innominate artery is the most common site.2, 4) In our case, the injury site was near the bifurcation and not the proximal part, and although this is a rare pattern, it had been previously documented.2)
In most cases, the injury pattern came out as a pseudoaneurysm of the innominate artery but some cases showed abrupt disruption or transection like our case.1-8) Some symptoms and signs were also different depending on the injury pattern; shock with hemoptysis, stable and equal blood pressures bilaterally, or blood pressure discrepancy between arms, dyspnea, cough, hypoxia, chest pain, stridor, gross facial and right upper limb swelling, and so on.1-8) But they showed common signs such as widening of mediastinum, extensive hemorrhage or hematoma along the arch and around the aortic branches.2, 4) As well as the injury of the innominate artery, other associated injuries can also be found, such as other aortic branch or aorta injuries, cervical vertebra, ribs, clavicle and sternum fractures, trachea-bronchial injury, and pneumothoraces.1-3, 5-7) When the injury of the innominate artery is presented as a pseudoaneurysm and the diagnosis and urgent treatment is delayed, critical complication can follow as the pseudoaneurysmal rupture or thromboembolism occurs.3) But these symptoms can be nonspecific and it may be difficult to anticipate the injury of the innominate artery as our case has shown. Other documented cases also revealed that an accurate diagnosis with appropriate treatment can be delayed or missed even up to 17 years after trauma.3, 4, 6, 8) In our case, the deceased showed no specific sign to suspect this injury and he had no blunt trauma or deceleration injury history, even though he complained of neck pain, cough, transient dyspnea, and loss of consciousness before admission. We assumed that these symptoms would be related to pseudoaneurysm of the innominate artery and consequently, he suddenly died of disruption of the pseudoaneurysm.
Most documented cases are related to clinical reviews where the injury pattern which is pathologically described was not previously known. The known pathologic findings of the innominate artery injury are various.4) The intimal disruption or injury with varying degrees and the media with or without pseudoaneurysm is the most common type of injury.4) In our case, the intima and media were transected and the arterial wall was partly avulsed from the surrounding connective tissue, which was regarded as an avulsion injury. Eventually, enormous hemorrhage followed the injury, extending to neck, both the pleural cavity and the mediastinum, and around aorta and aortic branches. Therefore, we suggest that, when extensive hemorrhage or hematoma is identified on neck and mediastinum with or without hemothorax during procedure, aortic branches should also be examined as well as the aorta, regardless of the deceased's injury history. Dissection should be performed very carefully because it can be difficult to find the injury site because extensive hemorrhage can destroy the surrounding connective tissue and the injury of the innominate artery with a pattern of pseudoanerysm is more common than disruption or transection of the artery. As our case revealed, avulsion injury can be also identified around the artery. We hope that our method of approach is helpful in this regard and also believe that we could also take similar hints from surgery techniques in order to control bleeding, if the specific site of the injured artery is not found or a large hematoma is encountered, you can approach the vessel by dissecting along the aorta.2)
We presented an unusual case of traumatic injury of the innominate artery. The injury of the innominate artery usually caused by blunt trauma such as motor vehicle accidents and fall from height, with or without the associated injury. In cases without explicit trauma history and extensive hemorrhage in the neck, mediastinum, or aorta and aortic branches however, the postmortem examination should be performed carefully in order not to miss this injury.

 XML Download
XML Download