

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Transmesenteric hernia is a very rare condition of congenital or acquired disease, and is the very small group of internal hernias which are uncommon and are rare cause of intestinal obstruction. In a lot of English literatures reviewed, it usually occurred in childhood, especially in pediatric populations. The adult cases were even rarer. It usually shows nondiagnostic and nonspecific symptoms, such as constipation, and radiographic and laboratory studies show no significant findings, just only suggesting bowel obstruction related signs. It is often diagnosed in operative field of explorative-laparotomy to acute abdomen. Underdiagnosed or undiagnosed cases are sometimes seen in postmortem examination, in which a segment of bowel with gangrene or perforated small intestine is revealed. We report an autopsy case of transmesenteric hernia developed in an adolescent who was admitted to a hospital for acute abdomen and died in an unexpected sudden way while differential diagnostic processes for the deceased's abdominal pain was being performed.
Case Report
A 18-years-old boy, who had nothing significant in his past medical history, admitted the hospital for acute abdominal pain and nausea. His abdominal pain began 4 hours later after he had had a meal in the evening with his family. The vital signs were 168/94 mmHg (blood pressure), 118/min (pulse rate), 26/min (respiratory rate), 36.8℃ (body temperature) at the emergency room. The aggravated abdominal pain showed colicky pattern and localized tenderness in the periumbilical area. There was, however, no rebound tenderness on the patient's abdomen on medical staffs physical examination. The complete blood count (CBC) study showed a mild degree of leukocytosis (neutrophils 38%), normal platelet count (270 109/L), normal hemoglobin level (15.6 g/dL). Just a sign of small bowel ileus was noted in the simple abdomen X-rays. A CT scan of the patient's abdomen presented mesenteric haziness on the right lower area of the abdomen and air-fluid level formation in the small intestine. But there was no any definite feature of ischemia or infarction of the mesentery or intestine. While mesenteric lymphadenitis, minimal enteritis or vasculitis of the mesentery were clinically considered in differential diagnosis, fluid intravenous adminstration, injections of empirical antibiotics and analgesics treatment were done. The patient was not allowed any oral intake. His abdominal pain was, however, not relieved for twelve hours after admission and even a sudden loss of consciousness for a few seconds occurred. At that time, his blood pressure lowered to 66/48 mmHg and the heart rate was elevated over 150/min. A consecutive CBC study revealed severe leukocytosis (37.0 109/L). Though intensive care unit treatments followed for the vital unstableness and severe leukocytosis, organ failure signs including renal hypofunction developed and the patient died the next day after admission. Clinicians added food poisoning, mesenteric necrosis, acute pancreatitis, autoimmune disorder, hemolytic uremic syndrome and thrombotic thrombocytopenic purpura in the differential diagnosis of the illness, failing to diagnose the exact cause of the patient's acute abdomen.
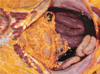
On autopsy, a long segment of the small intestine was found markedly engorged with dark black discoloration. There was about 2300 cc of bloodstained exudate in the peritoneal cavity (Fig. 1). The internal solid organs appeared pale. A small round defect of small bowel mesentery was seen at the pedicle of a portion of the mesentery (Fig. 2). The diameter of the mesenteric defect was about 3.5 cm, through which the ileum was herniated (Fig. 3). The herniated ileum was not covered with any memabranous sac tissue and in a torsional obstruction state with transmural hemorrhagic necrosis (Fig. 4). There was no significant disease or injury found accountable for the patient's death. Toxicologic study of the blood and gastric contents was unremarkable.
Discussion
Transmesenteric hernia is protrusion of viscera through a defect in the mesentery of small bowel, transverse or sigmoid colon and usually has no sac. It is a very rare condition and the literature on it consists largely of reports of isolated cases.1, 2) Transmesenteric hernia is a form of intestinal hernia. Intestinal hernia have been classified by Steinke as follows, and it will be noticed that the term "intestinal hernia"is applied to internal herniae of the peritoneal cavity only. The retroperitoneal herniae is categorized as four regions follows 1) paraduodenal, 2) paracecal, 3) intersigmoid and 4) foramen of Winslow. The second class of herniae is occurring through anomalous openings, and categorized as five regions 1) mesentery of small bowel, 2) mesentery of transverse colon, 3) mesentery of sigmoid colon, 4) omentum and 5) broad ligament. After Hensing was the first to describe the surgical anatomy of some varieties of internal herniae, many reports are described. Treitz gave his classical and detailed description of the para-duodenal fossae, which is very important region of the herniae, and the ligament of Treitz in that region continues to remind us of his contribution.1) Treves was the first to describe the various fossae and mesenteric defect in the ileocecal region and again has given his name to a structure in the region -the bloodless fold of Treves or Treves field, which is very important region of the herniae, too.1, 3)
There are many reports for internal herniae, and among the all herniae the transmesenteric hernia is 8~38% in prevalence, their age ranged from 12 to 86 years, but about 35% is occurred in childhood especially in pediatric period and are probably caused by a congenital mechanism.4) But transmesenteric hernia in adult and adolescent is very rare and sudden death case with transmesenteric hernia in the adult is barely reported either. On the literatures reported, there were few of sudden death by transmesenteric herniation in Korea and other countries.2, 5-7) Until present in Korea, the 2 autopsy cases were reported in infants under 5 years old. The victims of those reports showed just only nonspecific abdominal pain, and while clinical diagnosis could not be made in hospital management, the patients died suddenly.
The small bowel mesentery is a broad, fan-shaped fold of peritoneum that suspends the loops of the small intestine from the posterior abdominal wall.4) Herniation through the small bowel mesentery appears to be less common than herniation through the transverse mesocolon. Defect in the mesentery of the small bowel may be congenital or acquired. Congenital cases do not give a significant past history of trauma and a developmental origin of these defect is most probable. Three etiologic hypothesis have been proposed for congenital mesenteric defect: 1) partial regression of the dorsal mesentery 2) fenestration during the developmental enlargement of an inadequately vascularized area 3) an ileocecal mesentery with considerable and rapid lengthening in fetal life. Therefore the term "congenital"is not strictly correct as these defects may not be present at birth but develop later. The congenital defects are usually small being less than 5 cm across, and the majority lie in the ileal mesentery.1, 8) An acquired defect may follow after operation, trauma or inflammation. Post-operative herniations have been well described, the causes of which are now widely known and hence rare. The cases of inflammatory origin usually involve the ileocecal region. A case is reported which following appendicitis which had involved the mesentery of the terminal ileum leading to thrombosis of the adjacent vessels, a thinning of the mesentery and finally the presence of a hiatus.1)
It is known that preoperative diagnosis by routine clinical examination is very difficult. A mesenteric defect, with or without herniation of bowel through it may be symptomless, or symptoms may be so minor as to attract little or no attention. When obstruction or strangulation occurs, symptoms come on with dramatic suddenness and usually progress with great rapidly to a fatal issue. In the early phase of symptom onset, sudden, severe, colicky pain is the cardinal feature; vomiting occurs early, constipation is absolute and there are no physical signs. In later, visible peristalsis and abdominal distension may be present; a mass is only rarely felt. Bowel sounds are like those of intestinal obstruction; with perforation and peritonitis, paralytic ileus may supervene. The features developed in the late phase of transmesenteric hernia are those of intestinal obstruction, shock, and peritonitis when perforation has occurred. The duration of symptoms before hospital admission ranged from as little as 3 hours to as long as 3 months. A volvulus may further complicate the process and cause rapid hernial strangulation and intestinal gangrene, and over 50% of cases occurs gangrene.1, 4) Transmesenteric hernia usually manifests in association with proximal small bowel dilatation, with a transition zone to a normal or collapsed intestine. On opening the abdomen free fluid is always present. If strangulation has occurred the exudate is dark or bloodstained. If gangrene has supervened with bowel perforation, intestinal contents and pus will be present. The definitive treatment consists of reducing the hernia, resecting the bowel if not viable and repairing the defect.
The radiography studies are usually not helpful - the presence of dilated loops of bowel will only confirm the clinical diagnosis of intestinal obstruction, not mesenteric hernia. But recently imaging studies such as CT may play an important role if accurate and reliable CT findings can be obtained.4) Because the small bowel mesenteric defect itself is not visualized, observation of the clustering of small bowel loops and abnormalities of the mesenteric vessels play an important role in diagnosis of transmesenteric hernia. CT shows that the mesenteric vascular pedicle is characteristically engorged, stretched, and crowded; in addition, converging mesenteric vessels are located at the entrance of the hernial sac and there is displacement of the main mesenteric trunk.4) If strangulated, the configuration of the obstructed loop, mesenteric changes, and the enhancement patterns of the bowel wall can observed. The obstructed loop shows sac-like mass or cluster of dilated bowel loops. The mesentery shows engorged, stretched, and displaced mesenteric features. In addition the dilated bowel loops have converging vessels at the entrance of the hernial orifice, thus revealing the impaired venous drainage and continuous influx of the arterial flow.4, 9) But, despite of these findings, accurate diagnosis of hernia is still difficult.
The followings are regarded in a textbook10) as indications of surgical approach for acute abdomen ; 1) definite signs of peritonitis such as tenderness, guarding, and rebound tenderness, 2) severe or increasing localized tenderness, 3) abdominal pain and signs of sepsis not be explained by any other finding, 4) certain radigraphic finding consistent with pneumoperitoneum and intestinal perforation. Reviewing our case, was it really unnecessary to do a more aggressive surgical approach? There would be a lot of arguments among clinicians for whether the patient required aggressive surgical approach or not. We report a rare case of sudden death by transmesenteric hernia developed in adolescent - who admitted in hospital for acute abdomen and died unexpectedly and was finally diagnosed the cause of death on autopsy. In addition, it should be also admitted that accurate diagnosis of transmesenteric hernia is very difficult on the clinician basis. We present this case to wish that it would be helpful to clinicians to manage patients who present their clinical symptoms and signs like this presenting case.



 XML Download
XML Download