

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
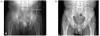
Primary hyperparathyroidism is mainly caused by parathyroid adenoma (85%) and is characterized by hypercalcemia, osteoporosis, renal stones, and gastrointestinal and neurological disorders. Because of improvements in blood analysis over the last two decades, primary hyperparathyroidism is typically diagnosed early and asymptomatically. A rare clinical manifestations of primary hyperparathyroidism, brown tumors (osteitis fibrosa cystica), are osteolytic lesions resulting from long-term hyperparathyroidism. Radiologically, it is difficult to distinguish a brown tumor from plasmacytoma, multiple myeloma, or bone metastasis. We report a case of a 44-year-old man with primary hyperparathyroidism that caused a large brown tumor (11 × 5 × 8 cm) that mimicked plasmacytoma or cancer metastasis on pelvic magnetic resonance imaging. After a bone biopsy report that was highly suggestive of a brown tumor, serum calcium and intact parathyroid hormone levels were determined. The lesion was ultimately diagnosed as a brown tumor and a parathyroidectomy was performed. After 1 year, the lesion has nearly regressed by follow up of the anteroposterior view of the pelvis and bone mineral density has improved. The present case highlights the importance of considering brown tumors in the evaluation of patients presenting with hypercalcemia and osteolytic lesions without definite primary neoplasm.
Figures and Tables
 | Fig. 1MRI in 44-year-old man with brown tumor in left pelvic bone (arrow). A. Sagittal T2-weighted image shows heterogeneous high signal mass in left pelvic bone. B. Sagittal T1-weighted image shows heterogeneous low signal mass in left pelvic bone. C. Gd enhanced scan shows diffuse enhancement in left pelvic bone.
|
 | Fig. 2Whole body bone scan shows increased technetium uptake on left ilium, left frontal bone, disital shaft of left humerus, mid-shaft of right tibia, T10 body and left femur (arrow).
|
 | Fig. 3
99mTc-MIBI parathyroid SPECT shows hot uptake in left thyroid bed (inferior portion) at 30 minutes and also at 3 hours.
|

References
1. Lee EJ, Lim SK, Park SS, Kang SW, Km HM, Lee HC, Park CS, Jeang HJ, Park IS, Huh KB. 5 cases of primary hyperparathyroidism. J Korean Med Assoc. 1988. 31:543–552.
2. Chung HK, Kim DY, Woo JT, Kim SW, Yang IM, Kim JW, Kim YS, Kim KW, Choi YK. Review of clinical characteristics of primary hyperparathyroidism. J Korean Soc Endocrinol. 1992. 7:234–242.
3. Diamanti-Kandarakis E, Livadas S, Tseleni-Balafouta S, Lyberopoulos K, Tantalaki E, Palioura H, Giannopoulos A, Kostakis A. Brown tumor of the fibula: unusual presentation of an uncommon manifestation. Report of a case and review of the literature. Endocrine. 2007. 32:345–349.
4. Hoshi M, Takami M, Kajikawa M, Teramura K, Okamoto T, Yanagida I, Matsumura A. A case of multiple skeletal lesions of brown tumors, mimicking carcinoma metastases. Arch Orthop Trauma Surg. 2008. 128:149–154.
5. Jouan A, Zabraniecki L, Vincent V, Poix E, Fournie B. An unusual presentation of primary hyperparathyroidism: severe hypercalcemia and multiple brown tumors. Joint Bone Spine. 2008. 75:209–211.
6. Mok JO. A case of brown tumor with severe hypercalcemia caused by parathyroid adenoma. J Korean Soc Endocrinol. 2003. 18:221–226.
7. Lee SK, Moon SD, Kim HS, Park EJ, Ahn SJ, Han JH, Kang MI, Cha BY, Lee KW, Son HY, Kang SK. A case of mediastinal parathyroid adenoma presenting as fracture of brown tumor. Korean J Med. 1999. 56:113–118.
8. Son HD, Woo JT, Kim SW, Yang IM, Kim JW, Kim YS, Kim KW, Choi YK. Increase of bone mineral density after surgical treatment of primary hyperparathyroidism. J Korean Soc Endocrinol. 1992. 7:76–79.
9. Tritos NA, Hartsband P. Rapid improvement of osteoporosis following parathyroidectomy in a premenopausal woman with acute primary hyperparathyroidism. Arch Intern Med. 1999. 159:1495–1498.
10. Nakaoka D, Sugimoto T, Kobayashi T, Yamaguchi T, Kobayashi A, Chihara K. Prediction of bone mass change after parathyroidectomy in patients with primary hyperparathyroidism. J Clin Endocrinol Metab. 2000. 85:1901–1907.
11. Silverberg SJ, Gartenberg F, Jacobs TP, Shane E, Siris E, Staron RB, McMahon DJ, Bilezikian JP. Increased bone mineral density after parathyroidectomy in primary hyperparathyroidism. J Clin Endocrinol Metab. 1995. 80:729–734.
12. Scott SN, Graham SM, Sato Y, Robinson RA. Brown tumor of the palate in a patient with primary hyperparathyroidism. Ann Otol Rhinol Laryngol. 1999. 108:91–94.
13. Daniels JS. Primary hyperparathyroidism presenting as a palatal brown tumor. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2004. 98:409–413.
14. Mundy GR, Cove DH, Fisken R. Primary hyperparathyroidism changes in the pattern of clinical presentation. Lancet. 1980. 1:1317–1320.
15. Khan A, Bilezikian J. Primary hyperparathyroidism: pathophysiology and impact on bone. CMAJ. 2000. 163:184–187.
16. Gupta A, Horattas MC, Moattari AR, Shorten SD. Disseminated brown tumors from hyperparathyroidism masquerading as metastatic cancer: a complication of parathyroid carcinoma. Am Surg. 2001. 67:951–955.
17. Heath H 3rd, Hodgson SF, Kennedy MA. Primary hyperparathyroidism. Incidence, morbidity, and potential economic impact in a community. N Engl J Med. 1980. 302:189–193.
18. Kim SZ, Park CH, Yoon SN, Kim BS, Chung YS. Brown tumors due to parathyroid carcinoma; 99mTc-MIBI scan findings: case report. Korean J Nucl Med. 1997. 31:395–398.
19. Blinder G, Hiller N, Gatt N, Matas M, Shilo S. Brown tumor in the cricoid cartilage: an unusual manifestation of primary hyperparathyroidism. Ann Otol Rhinol Laryngol. 1997. 106:252–253.
20. Ishibashi M, Nishida H, Hiromatsu Y, Kojima K, Uchida M, Hayabuchi N. Localization of ectopic parathyroid glands using technetium-99m sestamibi imaging: comparison with magnetic resonance and computed tomographic imaging. Eur J Nucl Med. 1997. 24:197–291.
 XML Download
XML Download