

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Persistent or recurrent primary hyperparathyroidism after initial parathyroid surgery occurs at rates of 1.5~10%. A single missed parathyroid adenoma accounts for the majority of persistent hyperparathyroidism, whereas metachronous parathyroid adenoma is a rare cause of recurrent hypercalcemia.
We report a case of a 39-year-old female who presented with recurrent pancreatitis. She had symptoms of hyperparathyroidism such as hypercalcemia, hypophosphatemia, hypercalciuria, nephrocalcinosis, and osteoporosis. She had a 2-cm firm neck mass under the right submandibular area. She was diagnosed with primary hyperparathyroidism 22 years ago. At that time, the right upper and lower parathyroid glands were removed after exploration of all parathyroid glands, and a right upper parathyroid adenoma was diagnosed. Now, she had a second surgery to remove the right submandibular mass with intraoperative PTH monitoring, which was diagnosed as a parathyroid adenoma in an ectopic supernumerary parathyroid gland. Because of hungry bone syndrome, she received calcium carbonate replacement therapy and has no evidence of recurrence. Here, we report a recurrent parathyroid adenoma in the undescended, supernumerary parathyroid gland after a long interval from the initial surgery.
Figures and Tables
Fig. 1
A. There is a diffuse parenchymal swelling with pseudocyst and peripancreatic infiltration in the tail of pancreas which is compatible with acute pancreatitis. B. In the kidney, bilateral renal medullary calcinosis is noted.
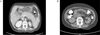
Fig. 2
A. There is a 2.2 × 1.2 cm sized circumscribed oval shaped multiseptated cystic mass in right submandibular area in the cervical ultrasound. B. About 2.6 cm measured ovoid solid mass in right submandibular space, attached to inferior portion of right submandibular gland is observed in the neck CT scan. C. The 20-minute image shows Tc-99m sestamibi uptake in the thyroid and a nodular mass in the right upper neck. In the 3-hour delayed image, the thyroid glands show less uptake, whereas the right upper neck mass shows more intense uptake.

Fig. 3
Microscopy of parathyroid adenoma shows partial hemorrhagic infarction. (H&E. ×2, ×40, ×100, ×400, clockwise). A. The tumor does not have well defined connective tissue capsule. Left upper portion shows massive hemorrhagic infarction. Lower cellular portion shows multinodular growth pattern. B. There is no vascular invasion, perineural space invasion or capsular penetration with growth into adjacent tissues, which are differential point from parathyroid carcinoma. C. The tumor shows hemorrhagic infarction. D. The chief cells are predominant and arranged in acinar pattern. The cytoplasm is either faintly eosinophilic or vacuolated. Nuclei are round, and have finely dense chromatin and inconspicuous nucleoli which corresponds to parathyroid adenoma.

References
1. Marx SJ. Hyperparathyroid and hypoparathyroid disorders. N Engl J Med. 2000. 343:1863–1875.
2. Chung HK, Kim DY, Woo JT, Kim SW, Yang IM, Kim JW, Kim YS, Kim KW, Choi YK. Review of clinical characteristics of primary hyperparathyroidism. J Korean Soc Endocrinol. 1992. 7:234–242.
3. Wang CA. Surgical management of primary hyperparathyroidism. Curr Probl Surg. 1985. 22:1–50.
4. Auguste LJ, Attie JN, Schnaap D. Initial failure of surgical exploration in patients with primary hyperparathyroidism. Am J Surg. 1990. 160:333–336.
5. Carneiro DM, Irvin GL 3rd. Late parathyroid function after successful parathyroidectomy guided by intraoperative hormone assay (QPTH) compared with the standard bilateral neck exploration. Surgery. 2000. 128:925–929.
6. Brennan MF, Nortan JA. Reoperation for persistent and recurrent hyperparathyroidism. Ann Surg. 1985. 201:40–44.
7. Weber CJ, Sewell CW, McGarity WC. Persistent and recurrent sporadic primary hyperparathyroidism: histopathology, complications, and results of reoperation. Surgery. 1994. 116:991–998.
8. Jaskowiak N, Norton JA, Alexander HR, Doppman JL, Shawker T, Skarulis M, Marx S, Spiegel A, Fraker DL. A prospective trial evaluating a standard approach to reoperation for missed parathyroid adenoma. Ann Surg. 1996. 224:308–320.
9. Yen TW, Wang TS, Doffek KM, Krzywda EA, Wilson SD. Reoperative parathyroidectomy: an algorithm for imaging and monitoring of intraoperative parathyroid hormone levels that results in a successful focused approach. Surgery. 2008. 144:611–619.
10. Adami S, Marcocci C, Gatti D. Epidemiology of primary hyperparathyroidism in Europe. J Bone Miner Res. 2002. 17:N18–N23.
11. Delbridge LW, Younes NA, Guinea AI, Reeve TS, Clifton-Bligh P, Robinson BG. Surgery for primary hyperparathyroidism 1962-1996: indications and outcomes. Med J Aust. 1998. 168:153–156.
12. Satava RM Jr, Beahrs OH, Scholz DA. Success rate of cervical exploration for hyperparathyroidism. Arch Surg. 1975. 110:625–628.
13. Haff RC, Ballinger WF. Causes of recurrent hypercalcemia after parathyroidectomy for primary hyperparathyroidism. Ann Surg. 1971. 173:884–891.
14. Clark OH, Way LW, Hunt TK. Recurrent hyperparathyroidism. Ann Surg. 1976. 184:391–402.
15. Martin JK Jr, van Heerden JA, Edis AJ, Dahlin DC. Persistent postoperative hyperparathyroidism. Surg Gynecol Obstet. 1980. 151:764–768.
16. Hedbäck G, Odén A. Recurrence of hyperparathyroidism: a long-term follow-up after surgery for primary hyperparathyroidism. Eur J Endocrinol. 2003. 148:413–421.
17. Kim YS, Koh SH, Koh YK, Park HC, Hong SH, Lee KH, Oh SM, Yoon C, Joo HZ. Clinical analysis of primary hyperparathyroidism. J Korean Surg Soc. 1997. 53:647–660.
18. Feingold DL, Alexander HR, Chen CC, Libutti SK, Shawker TH, Simonds WF, Marx SJ, Skarulis MC, Doppman JL, Schrump DS, Bartlett DL. Ultrasound and sestamibi scan as the only preoperative imaging tests in reoperation for parathyroid adenomas. Surgery. 2000. 128:1103–1109.
19. Irvin GL, Solorzano CC, Carneiro DM. Quick intraoperative parathyroid hormone assay: surgical adjunct to allow limited parathyroidectomy, improve success rate, and predict outcome. World J Surg. 2004. 28:1287–1292.
 XML Download
XML Download