

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
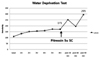
Post-obstructive diuresis after treatment for neurogenic bladder-induced obstructive kidney disease is a common symptom. As polyuria may develop in many other conditions as well, the present case is about a patient with a chief complaint of polyuria accompanied by nocturia, that was initially diagnosed as hydronephrosis due to the presence of neurogenic bladder and bladder dysfunction. The result of the water deprivation test, which was conducted for persistent diluted polyuria, yielded a final diagnosis of central diabetes insipidus, notwithstanding the strong impression of post-obstructive diuresis initially made because of a sudden increase in urine output after an indwelling catheter was inserted for bladder decompression.
In post-obstructive diuresis, polyuria actually does compensate for disturbed homeostasis through water and electrolyte diuresis and it does not require specific management. However, in central diabetes insipidus, which resembles manifestations of dilute polyuria, the urine and plasma osmolarity need to be under the strict control of anti-diuretic hormone. In the case of persistent dilute polyuria occurring after obstructive uropathy, underlying diseases such as diabetes insipidus should be taken into consideration.
Figures and Tables
Fig. 1
Kidney US. Ultrasonogram shows increased both kidneys in size and calyceal, renal pelvis dilatation. Bilateral ureters are dilated and bladder is distended. Also, bladder shows lobulated outer contour.

References
1. Nyman MA, Schwenk NM, Silverstein MD. Management of urinary retention: rapid versus gradual decompression and risk of complications. Mayo Clin Proc. 1997. 72:951–956.
2. Fauci AS, Braunwald E, Kasper DK, Hauser SL, Longo DL, Jameson JL, Loscalzo JL. Harrison's principles of internal medicine. 2008. 17th ed. New York: the McGraw-Hill Companies, Inc.;2218–2221.
3. Lee JW, Choi H, Oh SJ. Nephrogenic diabetes insipidus associated with nonobstructive dilatation of the urinary tract and voiding difficulty. Korean J Urol. 2008. 49:562–565.
4. Chang YY, Kim HU, Kim HD, Shin YS, Lee JM, Kim HS, Kim SK, Bang BK. A case of congenital nephrogenic diabetes insipidus with bilateral hydronephrosis and hydroureter. Korean J Nephrol. 2002. 21:1026–1031.
5. Park CY, Kim HS. Treatment of renal injury in a patient presenting pituitary diabetes insipidus associated with bilateral hydronephrosis: a case report. Korean J Urol. 1994. 35:74–81.
6. Korzets A, Sachs D, Gremitsky A, Gershkovitz R, Farrage G, Chlibowsky A, Erlich N. Unexplained polyuria and non-obstructive hydronephrosis in a urological department. Nephrol Dial Transplant. 2004. 19:2410–2412.
7. Kim HJ, Kang MY, Kim KW, Jeong HS, Kim HS, Kim SW, Kim SY. Retrospective observation of long-term clinical courses of idiopathic central diabetes insipidus in adults. J Korean Endocr Soc. 2006. 21:482–489.
8. Kim BW. Idiopathic central diabetes insipidus in adult. J Korean Endocr Soc. 2001. 16:185–189.
 XML Download
XML Download