

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Brown tumors are erosive bony lesions caused by chronic excessive secretion of parathyroid hormone. Since the introduction of routine calcium measurement, the diagnosis of hyperparathyroidism has usually been made in asymptomatic patients and as a result, brown tumors are rarely observed as an initial manifestation of hyperparathyroidism.
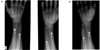
We report the case of a 70-year-old woman who presented with right wrist pain. A roentgenogram showed erosive bone tumors of the ulna and radius, which were mistaken for primary or metastatic bone tumors. Extensive workups were performed to determine the cause(s); however, these lesions were finally diagnosed as brown tumors associated with primary hyperparathyroidism due to a parathyroid adenoma. This case illustrates the diagnostic pitfall in patients who present with skeletal manifestations of hyperparathyroidism and the need for vigilance and a high level of suspicion by physicians.
Figures and Tables

References
1. Sulibuck JW, Perrier ND. Primary hyperparathyroidism. Oncologist. 2007. 12:644–653.
2. Diamanti-Kandarakis E, Livadas S, Tseleni-Balafouta S, Lyberopoulos K, Tantalaki E, Palioura H, Giannopoulos A, Kostakis A. Brown tumor of the fibula: unusual presentation of an uncommon manifestation. Report of a case and review of the literature. Endocrine. 2007. 32:345–349.
3. Hoshi M, Takami M, Kajikawa M, Teramura K, Okamoto T, Yanagida I, Matsumura A. A case of multiple skeletal lesions of brown tumors, mimicking carcinoma metastases. Arch Orthop Trauma Surg. 2008. 128:149–154.
4. Jouan A, Zabraniecki L, Vincent V, Poix E, Fournié B. An unusual presentation of primary hyperparathyroidism: severe hypercalcemia and multiple brown tumors. Joint Bone Spine. 2008. 75:209–211.
5. Mok JO. A case of brown tumor with severe hypercalcemia caused by parathyroid adenoma. J Korean Soc Endocrinol. 2003. 18:221–226.
6. Jung ST, Kim HJ, Lee DS, Park KH. Proximal humerus brown tumor with primary hyperparathyroidism in pregnancy. J Korean Bone Joint Tumor Soc. 2007. 13:173–179.
7. Chung HK, Kim DY, Woo JT, Kim SW, Yang IM, Kim JW, Kim YS, Kim KW, Choi YK. Review of clinical characteristics of primary hyperparathyroidism. J Korean Soc Endocrinol. 1992. 7:234–242.
8. Mackie GC, Schlicht SM. Accurate localization of supernumerary mediastinal parathyroid adenomas by a combination of structural and functional imaging. Australas Radiol. 2004. 48:392–397.
9. Yoon JH, Chang HS, Park CS. Surgical strategy in the management of primary hyperparathyroidism. J Korean Surg Soc. 2004. 66:372–378.
10. Kim SZ, Park CH, Yoon SN, Kim BS, Chung YS. Brown tumors due to parathyroid carcinoma; 99mTc-mibi scan findings: case report. Korean J Nucl Med. 1997. 31:395–398.
11. Wong LY, Wu CJ, Lin JC. Renal osteodystrophy. Zhonghua Yi Xue Za Zhi (Taipei). 1991. 47:342–349.
12. Kaya RA, Cavuşoğlu H, Tanik C, Kahyaoğlu O, Dilbaz S, Tuncer C, Aydin Y. Spinal cord compression caused by a brown tumor at the cervicothoracic junction. Spine J. 2007. 7:728–732.
13. Daniels JS. Primary hyperparathyroidism presenting as a palatal brown tumor. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2004. 98:409–413.
14. Blinder G, Hiller N, Gatt N, Matas M, Shilo S. Brown tumor in the cricoid cartilage: an unusual manifestation of primary hyperparathyroidism. Ann Otol Rhinol Laryngol. 1997. 106:252–253.
15. Scott SN, Graham SM, Sato Y, Robinson RA. Brown tumor of the palate in a patient with primary hyperparathyroidism. Ann Otol Rhinol Laryngol. 1999. 108:91–94.
16. Knezević G, Uglesić V, Kobler P, Svajhler T, Bagatin M. Primary hyperparathyroidism: evaluation of different treatments of jaw lesions based on case reports. Br J Oral Maxillofac Surg. 1991. 29:185–188.
17. Lee SK, Moon SD, Kim HS, Park EJ, Ahn SJ, Han JH, Kang MI, Cha BY, Lee KW, Son HY, Kang SK. A case of mediastinal parathyroid adenoma presenting as fracture of brown tumor. Korean J Med. 1999. 56:113–118.
18. Choi YW, OK CS. Brown tumor of the spine with compression fracture: a case report. J Korean Radiol Soc. 2006. 54:33–37.
19. Chung DW, Han CS, Park JY, Jeong ST. A brown tumor in metacarpal bone accompanied with primary hyperparathyroidism- a case report-. J Korean Soc Surg Hand. 2006. 11:66–71.
20. Hong WJ, Ku BJ, Lee JM, Han SW, Lee HJ, Rha SY, RO HK, Kim YK, Shong MH. A case of hyperparathyroidism presenting as brown tumor involving sacrum. Chungnam Med J. 2003. 30:283–288.
 XML Download
XML Download