

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
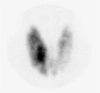
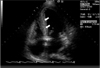
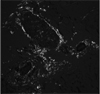
Amyloidosis is caused by deposition of insoluble amyloid protein in the extracellular space of organs and tissues. The causes of amyloidosis are classified as primary, secondary, and hereditary, and symptoms develop according to which organ is involved. Cardiac amyloidosis induces cardiomyopathy and is developed by deposition of amyloid proteins in cardiac tissue. We diagnosed a patient with rhabdomyolysis and thyrotoxicosis with underlying Graves' disease 5 years ago. The patient was readmitted recently complaining of general weakness and mild dyspnea, and was diagnosed as relapsed thyrotoxicosis. An echocardiogram was performed for the evaluation of dyspnea and the findings were compatible with infiltrative cardiomyopathy due to amyloidosis. A biopsy of the abdominal subcutaneous fat and rectal mucosa was performed, and diagnosis was amyloidosis with histologic findings. The cause of heart failure was therefore cardiac amyloidosis rather than thyrotoxicosis. This case indicates the importance of evaluating the cause of heart failure in patients with thyrotoxicosis.
Figures and Tables

References
1. Glenner GG. Amyloid deposits and amyloidosis. The beta-fibrilloses. N Engl J Med. 1980. 302:1283–1292.
2. Falk RH. Diagnosis and management of the cardiac amyloidoses. Circulation. 2005. 112:2047–2060.
3. Sanchorawala V. Light-chain(AL) amyloidosis: diagnosis × treatment. Clin J Am Soc Nephrol. 2006. 1:1331–1341.
4. Hong SB, Kim MS, Lee KW, Kim MR, In HH, Kim KR, Cho YU, Joo YC. Graves' disease associated with Hashimoto's thyroiditis. J Kor Soc Endocrinol. 1996. 11:182–188.
5. Siu SW, Yeung CY, Lau CP, Kung AWC, Tse HF. Incidence, clinical characteristics and outcome of congestive heart failure as the initial presentation in patients with primary hyperthyroidism. Heart. 2007. 93:483–487.
6. Klein I, Ojamaa K. Thyroid hormone and the cardiovascular system. N Engl J Med. 2001. 344:501–509.
7. Klein I, Ojamaa K. Thyrotoxicosis and the heart. Endocrinol Metab Clin North Am. 1998. 27:51–62.
8. Levey GS, Klein I. Catecholamine-thyroid hormone interaction and the cardiovascular manifestation of hyperthyroidism. Am J Med. 1990. 88:642–646.
9. Choudhury RP, MacDermot J. Heart failure in thyrotoxicosis, an approach to management. Br J Clin Pharmacol. 1998. 46:421–424.
10. Hassan W, Al-Sergani H, Mourad W, Tabbaa R. Amyloid heart disease. New frontiers and insights in pathophysiology, diagnosis, and management. Tex Heart Inst J. 2005. 32:178–184.
11. van Rijswijk MH, van Heusden CW. The potassium permanganate method. A reliable method for differentiating amyloid AA from other forms of amyloid in routine laboratory practice. Am J Pathol. 1979. 97:43–58.
12. Shenfield GM, Thompson J, Horn DB. Plasma and urinary digoxin in thyroid dysfunction. Eur J Pharmacol. 1977. 12:437–443.
13. Pollak A, Falk RH. Left ventricular systolic dysfunction precipitated by verapamil in cardiac amyloidosis. Chest. 1993. 104:618–620.
14. de Saedeleer B, Poppe K, Lacor P, de Mey J, Vincken W, Bourgain C, Velkeiniers B. Toxic intrathoracic goiter and mediastinal lymphadenopathy: an unusual presentation of systemic primary AL amyloidosis. Acta Clin Belg. 2003. 58:46–49.
15. Ikenoue H, Okamura K, Kuroda T, Sato K, Yoshinari M, Fujishima M. Thyroid amyloidosis with recurrent subacute thyroiditis-like syndrome. J Clin Endocrinol Metab. 1988. 67:41–45.
 XML Download
XML Download