

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Multiple endocrine neoplasia type 1 (MEN 1) is characterized by the combined occurrence of primary hyperparathyroidism, enteropancreatic tumors and anterior pituitary adenoma. Yet carcinoid tumors, adrenal adenoma and lipoma might exist simultaneously. Thymic carcinoid tumors, which are recognized as one of the causes of death for patients with MEN 1, are uncommon and their natural history has barely been investigated.
A 51-year-old man, who had undergone surgery and radiation therapy for thymic carcinoid tumor 15 years ago, was admitted to our hospital due to hypercalcemia that was detected on a routine health checkup. We found that he had hyperparathyroidism, a nonfunctioning pancreatic tumor and thyroid papillary microcarcinoma. We had studied the genetic alteration of the MEN 1 gene (menin) by using leukocyte genomic DNA. This genetic analysis clearly showed the missense mutation of the MEN 1 gene (V215M on exon 3). The thymic carcinoid tumor in this patient showed a relatively indolent course, in contrast to that for the ordinary MEN 1 patient, and this patient's thyroid papillary microcarcinoma was discovered incidentally. We present here this atypical case along with a review of the relevant literature.
Figures and Tables
Fig. 1
Thyroid sonography findings. A. Thyroid sonography showed about 1.2 × 0.7 cm sized low echogenic mass in the low portion of the right thyroid. B. About 1.1 × 1.2 cm sized low echogenic mass was found in the upper portion of the left thyroid.

Fig. 2
Parathyroid gland scintigraphy using 99mTc-sestamibi. A. The early image (10 min) showed a nodular hot uptake in the middle portion of the right thyroid, upper and lower poles of the left thyroid gland. B. In delayed image (2 hours), there was a hot uptake in the lower pole of the right thyroid gland.
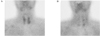
Fig. 3
Abdominal dynamic computed tomography. A. A large mass (6.8 cm) was noted in left paraaortic and subphrenic space on pre-enhance phase image. B. It was well-circumscribed, large hypervascular mass with heterogeneous high enhancement on arterial phase image.

Fig. 4
Histologic feature of thyroid papillary carcinoma and parathyroid gland. A. Low power view showed focus of micropapillary thyroid carcinoma having the classic papillary growth pattern (H & E stain, ×100). B. The parathyroid adenoma was composed mainly of chief cells. They had uniformly round nuclei and a moderate amount of cytoplasm (H & E stain, ×100).


References
1. Trump D, Farren B, Wooding C, Pang JT, Besser GM, Buchanan KD, Edwards CR, Heath DA, Jackson CE, Jansen S, Lips K, Monson JP, O'Halloran D, Sampson J, Shalet SM, Wheeler MH, Zink A, Thakker RV. Clinical studies of multiple endocrine neoplasia type 1 (MEN 1). QJM. 1996. 89:653–669.
2. Chandrasekharappa SC, Guru SC, Manickam P, Olufemi SE, Collins FS, Emmert-Buck MR, Debelenko LV, Zhuang Z, Lubensky IA, Liotta LA, Crabtree JS, Wang Y, Roe BA, Weisemann J, Boguski MS, Agarwal SK, Kester MB, Kim YS, Heppner C, Dong Q, Spiegel AM, Burns AL, Marx SJ. Positional cloning of the gene for multiple endocrine neoplasia-type 1. Science. 1997. 276:404–407.
3. Friedman E, Sakaguchi K, Bale AE, Falchetti A, Streeten E, Zimering MB, Weinstein LS, McBride WO, Nakamura Y, Brandi ML. Clonality of parathyroid tumors in familial multiple endocrine neoplasia type 1. N Engl J Med. 1989. 321:213–218.
4. Dong Q, Debelenko LV, Chandrasekharappa SC, Emmert-Buck MR, Zhuang Z, Guru SC, Manickam P, Skarulis M, Lubensky IA, Liotta LA, Collins FS, Marx SJ, Spiegel AM. Loss of heterozygosity at 11q13: analysis of pituitary tumors, lung carcinoids, lipomas and other uncommon tumors in subjects with familial multiple endocrine neoplasia type 1. J Clin Endocrinol Metab. 1997. 82:1416–1420.
5. Morelli A, Falchetti A, Martineti V, Becherini L, Mark M, Friedman E, Brandi ML. MEN1 gene mutation analysis in Italian patients with multiple endocrine neoplasia type 1. Eur J Endocrinol. 2000. 142:131–137.
6. Lemos MC, Thakker RV. Multiple endocrine neoplasia type 1(MEN1): Analysis of 1336 mutations reported in the first decade following identification of the gene. Hum Mutat. 2008. 29:22–32.
7. Tanaka C, Yoshimoto K, Yamada S, Nishioka H, Ii S, Moritani M, Yamaoka T, Itakura M. Absence of germ-line mutations of the multiple endocrine neoplasia type 1 (MEN1) gene in familial pituitar adenoma in contrast to MEN1 in Japanese. J Clin Endocrinol Metab. 1998. 83:960–965.
8. Marx SJ, Agarwal SK, Kester MB, Heppner C, Kim YS, Skarulis MC, James LA, Goldsmith PK, Saggar SK, Park SY, Spiegel AM, Burns AL, Debelenko LV, Zhuang Z, Lubensky IA, Liotta LA, Emmert-Buck MR, Guru SC, Manickam P, Crabtree J, Erdos MR, Collins FS, Chandrasekharappa SC. Multiple endocrine neoplasia type 1: Clinical and genetic features of the hereditary endocrine neoplasias. Recent Prog Horm Res. 1999. 54:397–438.
9. Brandi ML, Gahel RF, Angeli A, Bilezikian JP, Beck-Peccoz P, Bordi C, Conte-Devoix B, Falchetti A, Gheri RG, Libroia A, Lips CJ, Lombardi G, Mannelli M, Pacini F, Ponder BA, Raue F, Skogseid B, Tamburrano G, Thakker RV, Thompson NW, Tomassetti P, Tonelli F, Wells SA Jr, Marx SJ. Guidelines for Diagnosis and Therapy of MEN Type 1 and Type 2. J Clin Endocrinol Metab. 2001. 86:5658–5671.
10. Rosai J, Higa E, Davie J. Mediastinal endocrine neoplasm in patients with multiple endocrine adenomatosis: a previously unrecognized association. Cancer. 1972. 29:1075–1083.
11. Wilkinson S, Teh BT, Davey KR, McArdle JP, Young M, Shepherd JJ. Cause of death in multiple endocrine neoplasia type 1. Arch Surg. 1993. 128:683–690.
12. Shepherd JJ. The natural history of multiple endocrine neoplasia type I. highly uncommon or highly unrecognized? Arch Surg. 1991. 126:935–952.
13. Gibril F, Chen YJ, Schrump DS, Vortmeyer A, Zhuang Z, Lubensky IA, Reynolds JC, Louie A, Entsuah LK, Huang K, Asgharian B, Jensen RT. Prospective study of thymic carcinoids in patients with multiple endocrine neoplasia type 1. J Clin Endocrinol Metab. 2003. 88:1066–1081.
14. Kim HJ, Kim CS, Je HC, Park J, Park JS, Kong JH, Kang ES, Ahn CW, Cha BS, Lim SK, Kim KR, Lee HC, Jang HS, Hong SW. A case of multiple endocrine neoplasia type 1 with papillary thyroid carcinoma. J Kor Soc Endocrinol. 2006. 21:79–84.
15. Vortmeyer AO, Lubensky IA, Skarulis M, Li G, Moon YW, Park WS, Weil R, Barlow C, Spiegel AM, Marx SJ, Zhuang Z. Multiple endocrine neoplasia type 1: atypical presentation, clinical course, and genetic analysis of multiple tumors. Mod Pathol. 1999. 12:919–924.
16. Desai D, McPherson LA, Higgins JP, Weigel RJ. Genetic analysis of a papillary thyroid carcinoma in a patient with MEN 1. Ann Surg Oncol. 2001. 8:342–346.
17. Larsson C, Skogseid B, Oberg K, Nakamura Y, Nordenskjold M. Multiple endocrine neoplasia type 1 gene maps to chromosome 11 and is lost in insulinoma. Nature. 1988. 332:85–87.
18. Poisson A, Zablewska B, Gaudray P. Menin interacting proteins as clues toward the understanding of multiple endocrine neoplasia type 1. Cancer Lett. 2003. 189:1–10.
19. La P, Desmond A, Hou Z, Silva AC, Schnepp RW, Hua X. Tumor suppressor menin: the essential role of nuclear localization signal domains in coordinating gene expression. Oncogene. 2006. 25:3537–3546.
20. Hoff AO, Cote GJ, Gagel RF. Multiple endocrine neoplasias. Annu Rev Physiol. 2000. 62:377–411.
 XML Download
XML Download