

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Primary central nervous system (CNS) lymphoma is an uncommon neoplasm. However, the incidence of primary CNS lymphoma has increased more than 10-fold over the past three decades, and continues to accelerate. Currently, primary CNS lymphoma represents 4 to 7 percent of all newly diagnosed primary CNS tumors. Primary CNS lymphoma may arise from different parts of the brain, with deep hemispheric periventricular white matter being the most common site of origin. The presenting symptoms in primary CNS lymphoma vary depending on the location of the mass. Involvement of the hypothalamic-pituitary axis may cause hypopituitarism, diabetes insipidus, headache, diplopia, and blurred vision.
We experienced a case of a 58-year-old woman who developed central diabetes insipidus and panhypopituitarism secondary to primary CNS lymphoma. Hypothalamic and thalamic involvement were suspected based on brain MRI, and primary CNS lymphoma was confirmed by a CT-guided stereotactic biopsy. Through performing a water deprivation test and a combined pituitary stimulation test, we diagnosed complete type central diabetes insipidus and panhypopituitarism. Symptomatic relief was obtained with desmopressin, levothyroxine, hydrocortisone, and high-dose methotrexate-based chemotherapy. The thalamic and hypothalamic masses were significantly decreased in size after chemotherapy. We report the details of this case along with a review of the literature concerning primary CNS lymphom
Figures and Tables
Fig. 1
Homogeneously well enhancing mass lesion was noted in bilateral medial thalamus and hypothalamus on T1-weighted image. Extension into bilateral optic chiasm and proximal optic nerve was suspected. Minimal surrounding brain parenchymal edema was noted. Pituitary stalk was thickened.
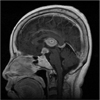
Fig. 2
Microscopic section from a tumor specimen. A. The tumor cells were pleomorphic with large nuclei and a coarse chromatin pattern. Tumor cells were clustered around a cerebral blood vessel in a pattern typical for primary central nervous system lymphoma. (hematoxylin and eosin stain, ×400). B. Tumor cells expressed the CD20 and showed dark membrane staining. (CD20 immunohistochemical stain, ×400)

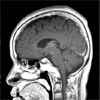
Fig. 3
After chemotherapy, brain MRI T1-weighted image showed decreased tumor size on both thalamus and hypothalamus, and diminished brain parenchymal edema.


References
1. Fine HA MR. Primary central nervous system lymphoma. Ann Intern Med. 1993. 119:1093–1104.
2. Batchelor T, Loeffler JS. Primary CNS lymphoma. J Clin Oncol. 2006. 24:1281–1288.
3. Erdag N, Bhorade RM, Alberico RA, Yousuf N, Patel MR. Primary lymphoma of the central nervous system: typical and atypical CT and MR imaging appearances. Am J Roentgenol. 2001. 176:1319–1326.
4. Kaufmann TJ, Lopes MB, Laws ER Jr, Lipper MH. Primary sellar lymphoma: radiologic and pathologic findings in two patients. Am J Neuroradiol. 2002. 23:364–367.
5. Liu JK, Sayama C, Chin SS, Couldwell WT. Extranodal NK/T-cell lymphoma presenting as a pituitary mass: case report and review of the literature. J Neurosurg. 2007. 107:660–665.
6. Silfen ME, Garvin JH Jr, Hays AP, Starkman HS, Aranoff GS, Levine LS, Feldstein NA, Wong B, Oberfield SE. Primary central nervous system lymphoma in childhood presenting as progressive panhypopituitarism. J Pediatr Hematol Oncol. 2001. 23:130–133.
7. Kim SH, Han DC, Park HM, Lee YB, Shin WC. A case of primary pituitary lymphoma. J Kor Neurol Assoc. 2006. 24:169–171.
8. Miller DC, Hochberg FH, Harris NL, Gruber ML, Louis DN, Cohen H. Pathology with clinical correlations of primary central nervous system non-Hodgkin's lymphoma: The Massachusetts General Hospital experience 1958-1989. Cancer. 1994. 74:1383–1397.
9. Hochberg FH, Miller DC. Primary central nervous system lymphoma. J Neurosurg. 1988. 68:835–853.
10. Ahsan H, Neugut AI, Bruce JN. Trends in incidence of primary malignant brain tumors in USA, 1981-1990. Int J Epidemiol. 1995. 24:1078–1085.
11. Nitta T, Kasuga C, Yasumoto Y, Okuda O, Kudo S, Sato K. A clinicopathological study of 21 cases of primary central nervous system lymphoma. No Shinkei Geka. 1994. 22:827–832.
12. Kim IM, Son EI, Kim DW, Yim MB, Kim SP. Treatment strategies for primary central nervous system lymphoma. J Kor Neurosurg Soc. 2001. 30:334–341.
13. Lee SH, Kim HS, Lee YM, Yoon YS, Lim SK, Lee HC, Huh KB. A case of central diabetes insipidus caused by metastatic malignant lymphoma. J Kor Endocrinol Soc. 1997. 12:596–601.
14. Kwak JW, Hong SH, Kim JH, Lee SH, Jo JH, Kwon HS, Youn KH, Cha BY, Son HY. A case of pituitary metastasis of breast cancer presenting as diabetes insipidus and panhypopituitarism. J Kor Endocrinol Soc. 2007. 22:125–129.
15. Rollins KE, Kleinschmidt-DeMasters BK, Corboy JR, Damek DM, Filley CM. Lymphomatosis cerebri as a cause of white matter dementia. Hum Pathol. 2005. 36:282–290.
16. Capra M, Wherrett D, Weitzman S, Dirks P, Hawkins C, Bouffet E. Pituitary stalk thickening and primary central nervous system lymphoma. J Neuro-Oncology. 2004. 67:227–231.
 XML Download
XML Download