

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Bisphosphonate-related osteonecrosis of the jaw (BRONJ) is a rare, but serious, side effect of bisphosphonate therapy that produces significant morbidity in affected patients. It is characterized by poor wound healing and spontaneous intra-oral soft tissue breakdown, which lead to exposure of necrotic maxillary and mandibular bone.
We report a case of BRONJ in 56-year-old man who visited Ajou University Hospital Dental Clinic in March 2007. He had been diagnosed with Waldenstrom's macroglobulinemia in 2005 and had been treated with chemotherapeutic agents, along with concomitant pamidronate injections (45 mg monthly). The patient had clinical features of bisphosphonate-related osteonecrosis of the mandible precipitated by tooth extraction. The patient had multiple systemic risk factors, including extended duration of intravenous pamidronate therapy, chemotherapy, and glucocorticoid therapy for his malignancy. In the 6 months prior to presentation, curettage and debridement were performed repeatedly, but there was no improvement in the mandibular lesion. The patient was referred to the Endocrinology Clinic and was diagnosed with BRONJ. We discontinued pamidronate and started conservative care. BRONJ should be considered in the differential diagnosis when patients complain of poor oral wound healing or have recurrent exposure of necrotic maxillary and mandibular bone.
Figures and Tables
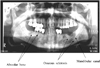 | Fig. 1A dental panoramic view demonstrated osseous sclerosis of alveolar bone in both sides of mandible. Mandibular canals were accentuated by surrounding osseous sclerosis.
|

References
1. Saad F, Lipton A. Clinical benefits and considerations of bisphosphonate treatment in metastatic bone disease. Semin Oncol. 2007. 34:Suppl 4. S17–S23.
2. Owens G, Jackson R, Lewiecki EM. An integrated approach: bisphosphonate management for the treatment of osteoporosis. Am J Manag Care. 2007. 13:Suppl 11. S290–S308.
3. Diel IJ, Bergner R, Grotz KA. Adverse effects of bisphophonates: current issues. J Support Oncol. 2007. 5:475 –482.
4. Marx RE. Pamidronate (AREDIA) and zoledronate (ZOMETA) induced avascular necrosis of the jaws: A growing epidemic. J Oral Maxillofac Surg. 2003. 61:1115 –1118.
5. Advisory Task Force on Bisphosphonate-Related Osteonecrosis of the Jaws, American Association of Oral and Maxillofacial Surgeons: American Association of Oral and Maxillofacial Surgeons position paper on bisphosphonate-related osteonecrosis of the jaws. J Oral Maxillofac Surg. 2007. 65:369–376.
6. Khosla S, Burr D, Cauley J, Dempster DW, Ebeling PR, Felsengerg D, Gagel RF, Gilsanz V, Guise T, Koka S, McCauley LK, McGowan J, McKee MD, Mohla S, Pendrys DG, Raisz LG, Ruggiero SL, Shafer DM, Shum L, Silverman SL, Poznak CHV, Watts N, Woo SB, Shane E. Bisphosphonate-Associated Osteonecrosis of the Jaw: Report of a Task Force of the American Society for Bone and Mineral Research. J Bone Miner Res. 2007. 22:1479–1491.
7. Park YJ, Pyo SW, Kim JA, Min JK. A case of avascular necrosis of mandible associated with the use of bisphosphonate in a patient with rheumatoid arthritis and osteoporosis. J Kor Rheum. 2006. 13:150–154.
8. Kwon YD, Yoon BW, Walter C. Bisphosphonate, is it an emerging risk factor in oral surgery? J Kor Maxillofac Plastic Recon Surg. 2007. 29:456–462.
9. Mavrokokki A, Cheng A, Stein B, Gross A. Nature and frequency of bisphosphonate-associated osteonecrosis of the jaws in Australia. J Oral Maxillofac Surg. 2007. 65:415–756.
10. Yarom N, Yahalom R, Shoshani Y, Hamed W, Regev E, Elad S. Osteonecrosis of the jaw induced by orally administered bisphosphonates: incidence, clinical features, predisposing factors and treatment outcome. Osteoporos Int. 2007. 18:1363–1370.
11. Marx RE. . Oral & intravenous bisphosphonate-induced osteonecrosis of the jaws: History, etiology, prevention, and treatment. 2007. IL, USA: Quintessence Publishing;77–95.
12. Woo SB, Hellstein JW, Kalmar JR. Systematic review: bisphosphonate and osteonecrosis of the jaws. Ann Intern Med. 2006. 144:753–761.
13. Lam DK, Sandor GK, Holmes HI, Evans AW, Clokie CM. A review of bisphosphonate-associated osteonecrosis of the jaws and its management. J Can Dent Assoc. 2007. 73:417–422.
14. Reid IR, Bolland MJ. Is bisphosphonate-associated osteonecrosis of the jaw caused by soft tissue toxicity? Bone. 2007. 41:318–320.
15. Phal PM, Myall RW, Assael LA, Weissman JL. Imaging findings of bisphosphonate-associated osteonecrosis of the jaws. Am J Neuroradiol. 2007. 28:1139–1145.
16. Wilkinson G, Kuo YF, Freeman KJ, Goodwin JS. Intravenous bisphosphonate therapy and inflammatory conditions or surgery of the jaw: A population-based analysis. J Natl Cancer Inst. 2007. 99:1016–1024.
 XML Download
XML Download