

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Although hematoma formation after fine needle aspiration cytology fine needle aspiration cytology (FNAC) is a most common complication and most of these hematomas are self-limiting with minimal pain, a massive intra-thyroidal hemorrhage that produces acute airway obstruction had rarely been reported on.
A 60-year old female underwent ultrasound-guided FNAC for evaluation of nodules that were in the right lobe (0.5 cm) and left lobe (3 cm) of her thyroid gland. Two hours later, the patient experienced swelling and progressive pain in the anterior neck. She visited an emergency room with dyspnea at 6 hours after FNAC. On the initial examination, her vital signs were stable and the oxygen saturation was 100%. On physical examination, her thyroid gland was tender and diffusely enlarged. Neck CT revealed diffuse enlargement of the thyroid gland with heterogeneous hyper-attenuated areas that were suspicious for intra-thyroidal hemorrhage and a highly enhanced area in the left lower lobe of the thyroid. No definite bleeding focus was identified on the angiography that was done through the carotid artery, but the left superior thyroid artery was severely congested and partial embolization was done. After embolization her neck pain and tenderness decreased over several days and the patient was discharged on the 6th hospital day. We report here on a case of diffuse hemorrhage into the thyroid gland after FNAC, and this was successfully treated with arterial embolization.
Figures and Tables
Fig. 1
CT of chest and neck. A. Chest CT revealed calcified nodule in left lower lobe of thyroid. B. Neck CT without contrast-enhancement revealed diffuse enlargement of thyroid gland with heterogeneous hyper-attenuated area suspicious for intra thyroidal hemorrhage. C. Neck CT with enhancement revealed diffusely enhanced thyroid gland with highly enhanced area in left lower lobe of thyroid.

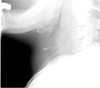
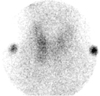
Fig. 3
Angiogram of left inferior thyroid artery. No definite bleeding focus was noted. Arrow indicated left inferior thyroid artery.

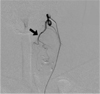
Fig. 4
Angiogram of left external carotid artery. Left superior thyroid artery was severely congested and partial embolization was done by particle via micro catheter. Arrow indicated left superior thyroid artery.
References
1. Mackenzie EJ, Mortimer RH. Thyroid nodules and thyroid cancer. Med J Aust. 2004. 180:242–247.
2. Belfiore A, La Rosa GL. Fine needle aspiration biopsy of the thyroid. Endocrinol Metab Clin North Am. 2001. 30:361–400.
3. Roh JL. Intrathyroid hemorrhage and acute upper airway obstruction after fine needle aspiration of the thyroid gland. Laryngoscope. 2006. 116:154–156.
4. Kim JH, Wi MW, Hong YH, Lee SY. A case of diffuse intracapsular hemorrhage of thyroid gland after fine needle aspiration biopsy. Korean J of Otolaryngo. 2007. 50:178–181.
5. Noordzij JP, Goto MM. Airway compromise caused by hematoma after thyroid fine-needle aspiration. Am J Otolaryngol. 2005. 26:398–399.
6. Gauger PG, Guinea AI, Reeve TS, Delbridge LW. The spectrum of emergency admissions for thyroidectomy. Am J Emerg Med. 1999. 17:591–593.
7. Shinohara S, Yamamoto E, Tanabe M, Maetani T, Kim T. Implantation metastasis of head and neck cancer after fine needle aspiration biopsy. Auris Nasus Larynx. 2001. 28:377–380.
8. Panunzi C, Paliotta DS, Papini E, Petrucci L, Rinaldi R, Nardi F. Cutaneous seeding of a follicular thyroid cancer after fine needle aspiration biopsy? Diagn Cytopathol. 1994. 10:156–158.
9. Ito Y, Asahi S, Matsuzuka F, Nakamura Y, Amino N, Miyauchi A. Needle tract implantation of follicular neoplasm after fine needle aspiration biopsy: report of a case. Thyroid. 2006. 16:1059–1062.
10. Tsang K, Duggan MA. Vascular proliferation of the thyroid. A complication of fine-needle aspiration. Arch Pathol Lab Med. 1992. 116:1040–1042.
11. Gordon DL, Gattuso P, Castelli M, Bayer W, Emanuele MA, Brooks MH. Effect of fine needle aspiration biopsy on the histology of thyroid neoplasm. Acta Cytol. 1993. 37:651–654.
12. Tomoda C, Takamura Y, Ito Y, Miya A, Miyauchi A. Transient vocal cord paralysis after fine needle aspiration biopsy of after thyroid tumor. Thyroid. 2006. 16:697–699.
13. Kim TY, Yang HM, Hwang JK. A case of acute suppurative thyroiditis as a complication of acupuncture in patient with a benign thyroid nodule. J Korean Soc Endocrinol. 2002. 17:576–582.
14. Isenberg SF. Thyroid abscess resulting from fine needle aspiration. Otolaryngol Head Neck Surg. 1994. 111:832–833.
15. Frates MC, Benson CB, Doubliet PM, Cibas ES, Marqusee E. Can color doppler sonography aid in the prediction of malignancy of thyroid nodules? J Ultrasound Med. 2003. 22:127–131.
16. Lampe HB, Cramer HM. Advances in the use of fine-needle aspiration cytology in the diagnosis of palpable lesion of the head and neck. J Otolaryngol. 1991. 20:108–116.
17. Martin HE, Ellis EB. Biopsy by needle puncture and aspiration. Ann Surg. 1930. 92:169–181.
18. Rizzatto G, Solibiati L, Croce F, Derchi LE. Aspiration biopsy of superficial lesions: ultrasonic guidance with a linear-array probe. Am J Roentgenol. 1987. 148:623–625.
19. Boey J, Hsu C, Collins RJ, Wong J. A prospective controlled study of fine needle aspiration and Tru-cut needle biopsy of dominant thyroid nodules. World J Surg. 1984. 8:458–465.
 XML Download
XML Download