

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Idiopathic central diabetes insipidus is most likely to occur in young patients who have a clinical history of autoimmune disease. The presentation of clinical findings such as central diabetes insipidus and pituitary stalk thickening on sellar magnetic resonance imaging (MRI) in a young women would strongly suggest lymphocytic hypophysitis, which is a rare inflammatory process involving the pituitary stalk and the pituitary gland, yet this disease can sometimes regress.
We describe here a young woman with lymphocytic hypophysitis. She suffered from an abrupt onset of central diabetes insipidus. Sellar MRI showed thickening of pituitary stalk and loss of high signal of normal neurohypophysis on T1-weighted image. Combind pituitary stimuation test showed a blunted response of GH.
To avoid the potential detrimental complications of invasive diagnostic procedures for testing the pituitary function in a fertile unmarried young woman, we chose close clinical and radiologic follow-up in the proper clinical context. The requirement for DDAVP was slightly decreased over time and the MR imaging obtained serially for 6 months revealed spontaneous partial regression of the pituitary lesion.
Figures and Tables
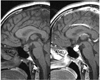 | Fig. 1Sellar MRI at admission. The normal posterior 'bright spot' on T1 weighted image is lost and pituitary gland is enlarged. Pituitary stalk is thickened with marked contrast enhancement.
|
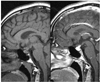 | Fig. 2Sellar MRI after 45 days later. Previous Pituitary enlargement and Pituitary Stalk thickening was regressed 6.6 mm to 4.6 mm.
|
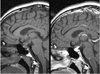 | Fig. 3Sellar MRI after 6 months later. Previous Pituitary enlargement and Pituitary Stalk thickening was more regressed 4.6 mm to 4.29 mm.
|

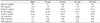
Table 3
Combined pituitary stimulation test after 6 months later

Using the same abbreviations on table 2.
![]()
References
1. Pivonello R, De Bellis A, Faggiano A, Di Salle F, Petretta M, Di Somma C, Perrino S, Altucci P, Bizzarro A, Bellastella A, Lombardi G, Colao A. Central diabetes insipidus and autoimmunity. J Clin Endocrinol Metab. 2003. 88:1629–1636.
2. Baik SH, Kim DS, Sung YK, Kim JP, Lee CB, Park YS, Choi WH, Ahn YH, Kim TW, Ko Y, Park MH. A case of lymphocytic hypophysitis in a postmenopausal woman. J Kor Endocr Soc. 2002. 17:713–719.
3. Lee SJ, Lee HL, Chung IK, Hong EG, Choi CS, Kim HK, Kim DM, Yoo JM, Ihm SH, Choi MG, Yoo HJ, Park SW. Lymphocytic hypophysitis associated with pregnancy. J Kor Endocr Soc. 2002. 17:705–712.
4. Son JM, Ko SH, Ahn YB, Ju K, Lee JR, Yang SE, Song KH, Son HY, Jun JS. A case of lymphocytic hypophysitis presented with hypoglycemia after delivery. J Kor Endocr Soc. 2003. 18:325–331.
5. Caturegli P, Newschaffer C, Olivi A, Pomper MG, Burger PC, Rose NR. Autoimmune hypophysitis. Endocr Rev. 2005. 26:599–614.
6. Kojima H, Nojima T, Nagashima K, Ono Y, Kudo M, Ishikura H. Diabetes insipidus caused by lymphocytic infundibuloneurohypophysitis. Arch Pathol Lab Med. 1989. 113:1399–1401.
7. Carol CC, Shereen E, Harley SS, Sylvia L. The spectrum and significance of primary hypophysitis. J Clin Endocrinol Metab. 2001. 86:1048–1053.
8. Imura H, Nakao K, Shimatsu A, Ogawa Y, Sando T, Fujisawa I, Yamabe H. Lymphocytic infundibuloneurohypophysitis as a cause of central diabetes insipidus. N Engl J Med. 1993. 329:683–689.
9. Rivera JA. Lymphocytic hypophysitis: Disease spectrum and approach to diagnosis and therapy. Pituitary. 2006. 9:35–45.
10. Jo YS, Lee HJ, Rha SY, Hong WJ, Song CJ, Kim YK, Ro HK. Lymphocytic hypophysitis with diabetes insipidus: Improvement by methylprednisolone pulse therapy. Korean J Intern Med. 2004. 19:189–192.
11. Unluhizarci K, Bayam F, Colak R, Ozturk F, Selcuklu A, Durak AC, Kelestimur F. Disctinct radiological and clinical appearance of lymphocytic hypophysitis. J Clin Endocrinol Metab. 2001. 86:1861–1864.
12. Goudie RB, Pinkerton PH. Anterior hypophysitis and Hashimoto's disease in a young woman. J Pathol Bacteriol. 1962. 83:584–585.
13. Pestell RG, Best JD, Alford FP. Lymphocytic hypophysitis: the clinical spectrum the disorder and evidence for an autoimmune pathogenesis. Clin Endocrinol. 1990. 33:457–466.
14. Lim DJ, Chung YG, Lee HK, Lee KC, Suh JK. Lymphocytic hypophysitis: A Case Report. J Korean Neurosurg Soc. 1998. 27:1611–1614.
15. Honegger J, Fahlbusch R, Bornemann A, Hensen J, Buchfelder M, Muller M, Nomikos P. Lymphocytic and granulomatous hypophysitis: Experience with nine cases. Neurosurgery. 1997. 40:713–723.
16. Tien RD, Newton TH, McDermott MW, Dillon PW, Kucharczyk J. Thickened pituitary stalk on MR images in patients with diabetes insipidus and Langerhans cell histiocytosis. Am J Neuroradiol. 1990. 11:703.
17. Koshiyama H, Satio H, Yorita S, Koh T, Kanatsuna T, Nishimura K, Hayakawa K, Takahashi J, Hashimoto N. Lymphocytic hypophysitis presenting with iabetes insipidus: case report and literature review. Endocr J. 1994. 41:93–97.
18. Panicker HK, Janicic N, Nguyen D, Verbalis J. Presumed infundibuloneurohypophysitis: Unusual presentation in a postpartum patient. Am J Neuroradiol. 2005. 26:357–359.
 XML Download
XML Download