

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Papillary thyroid microcarcinoma (PTMC) is defined as being 1 cm or less in diameter. Although the prognosis of PTMC is known to be more favorable than that of papillary thyroid carcinoma greater than 1 cm in diameter, pathologic factors suggesting aggressiveness, such as multifocality and lymph node invasion, have been reported to be highly prevalent in PTMC. However, the rate of distant metastasis in patients with PTMC is very low. Many investigators have reported that initial distant metastasis was detected only in patients with PTMC greater than 0.4 cm in diameter, however these cases have involved only one organ, usually the lung. We report here on an extremely unusual case of solitary PTMC (0.3 cm in diameter) presenting multiple distant metastases at the time of diagnosis.
Figures and Tables

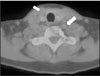
Fig. 2
Chest CT shows innumerable pulmonary metastatic nodules in both lungs and pericardial & right pleural effusions.

Fig. 3
Bone scan shows multiple bone metastasis in the C-spine, upper T-spine, L-spine, sacrum, bilateral pelvic bones, bilateral proximal femurs, and bilateral ribs.



References
1. Ito Y, Tomoda C, Uruno T, Takamura Y, Miya A, Kobayashi K, Matsuzuka F, Kuma K, Miyauchi A. Papillary microcarcinoma of the thyroid: How should it be treated? World J Surg. 2004. 28:1115–1121.
2. Baudin E, Travagli JP, Ropers J, Mancusi F, Brunobossio G, Caillou B, cailleux A, Lumbroso J, Parmentier C, Schlumberger M. Microcarcinoma of the thyroid gland. the Gustave-Roussy Institute experience. Cancer. 1998. 83:553–559.
3. Hay ID, Grant CS, van Heerden JA, Goellner JR, Ebersold JR, Bergstralh EJ. Papillary thyroid microcarcinoma: a study of 535 cases observed in a 50-year period. Surgery. 1992. 112:1139–1146.
4. Wada N, Duh QY, Sugino K, Iwasaki H, Kameyama K, Mimura T, Ito K, Takami H, Takanashi Y. Lymph node metastasis from 259 papillary thyroid microcarcinomas: frequency, pattern of occurrence and recurrence, and optimal strategy for neck dissection. Ann Surg. 2003. 237:399–407.
5. Chow SM, Law SC, Chan JK, Au SK, Yau S, Lau WH. Papillary microcarcinoma of the thyroid-Prognostic significance of lymph node metastasis and multifocality. Cancer. 2003. 98(1):31–40.
6. Pellegriti G, Scollo C, Lumera G, Regalbuto C, Vigneri R, Belfiore A. Clinical behavior and outcome of papillary thyroid cancers smaller than 1.5 cm in diameter: study of 299 cases. J Clin Endocrinol Metab. 2004. 89:3713–3720.
7. Roti E, Rossi R, Trasforini G, Bertelli F, Ambrosio MR, Busutti L, Pearce EN, Braverman LE, Degli Uberti EC. Clinical and histological characteristics of papillary thyroid microcarcinoma: Results of a retrospective study in 243 patients. J Clin Endocrinol Metab. 2006. 91:2171–2178.
8. Rosai J, LiVolsi VA, Sobrinho-Simoes M, Williams ED. Renaming papillary microcarcinoma of the thyroid gland: the Porto proposal. Int J Surg Pathol. 2003. 11:249–251.
9. Lee JD, Nam KH, Lim CY, Chung WY, Park CS. Differentiated thyroid carcinoma presenting distant metastasis as a initial sign. J Korean Surg Soc. 2006. 71:105–111.
10. Zubair W, Virginia A. Microcarcinoma of the thyroid. Adv Anat Pathol. 2006. 13:69–75.
11. Sakorafas George H, John G, Vania S. Papillary thyroid microcarcinoma: a surgical perspective. Cancer Treat Rev. 2005. 31:423–438.
12. Kasai N, Sakamoto A. New subgrouping of small thyroid carcinomas. Cancer. 1987. 60:1767–1770.
13. Roti E, Rossi R, Trasforini G, Bertelli F, Ambroso RM, Busutti L, Pearce EN, Braverman LE, Uberti EC. Clinical and histological characteristics of papillary thyroid microcarcinoma: Results of a retrospective study in 243 patients. J Clin Endocrinol Metab. 2006. 91:2171–2178.
14. Lee J, Rhee Y, Lee S, Ahn CW, Cha BS, Kim KR, Lee HC, Kim SI, Park CS, Lim SK. Frequent, aggressive behaviors of thyroid microcarcinomas in Korean patients. Endocr J. 2006. 53:627–632.
15. Pelizzo MR, Boschin IM, Toniato A, Pagetta C, Piotto A, Bernante P, Casara D, Pennelli G, Rubello D. Natural history, diagnosis, treatment and outcome of papillary thyroid microcarcinoma(PTMC): a mono -institutional 12-year experience. Nucl Med Commun. 2004. 25:547–552.
16. Mazzaferri EL, Robbins RJ, Spencer CA, Braverman LE, Pacini F, Wartofsky L, Haugen BR, Sherman SI, Cooper DS, Braunstein GD, Lee S, Davies TF, Arafah BM, Ladenson PW, Pinchera Al. A consensus report of the role of serum thyroglobulin as a monitoring method for low-risk patients with papillary thyroid carcinoma. J Clin Endocrinol Metab. 2003. 88:1433–1441.
17. Schelfhout LJ, Creutzberg CL, Hamming JF, Fleuren GJ, Smeenk D, Hermans J, van de Velde CJ, Goslings BM. Multivariate analysis of survival in differentiated thyroid cancer: The prognostic significance of the age factor. Eur J Cancer. 1988. 24:331–337.
18. Samaan NA, Schultz PN, Hickey RC, Goepfert H, Haynie TP, Johnston DA, Ordonez NG. The results of various modalities of treatment of well differentiated thyroid carcinoma: A retrospective review of 1599 patients. J Clin Endocrinol Metab. 1992. 75:714–720.
19. Strate SM, Lee EL, Childers JH. Occult papillary carcinoma of the thyroid with distant metastases. Cancer. 1984. 54:1093–1100.
 XML Download
XML Download